Download
1 / 41
410 likes | 630 Views
Dr. Ahmed Refaey. Shiny liver. FRCR. Consultant Radiologist Prince Sultan Military Medical City. Format of the lecture. Detection of liver masses by CT Hypervascular tumors of the liver Case of the day. Detection of liver masses by CT. * Triphasic study * arterial phase

E N D
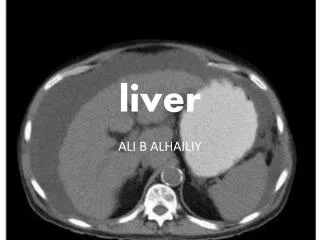
Dr. Ahmed Refaey Shiny liver FRCR Consultant Radiologist Prince Sultan Military Medical City
Format of the lecture • Detection of liver masses by CT • Hypervascular tumors of the liver • Case of the day
Detection of liver masses by CT * Triphasic study * arterial phase * portal venous phase * equilibrium phase ( delayed phase )
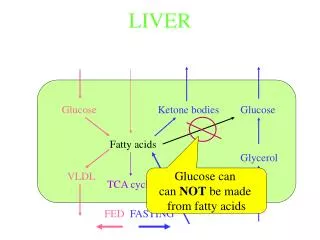
When we give IV contrast, it is important to understand that there is a dual blood supply to the liver. • Normal parenchyma is supplied for 80% by PV & only for 20% by hepatic artery, so it will enhance in the portal venous phase. • All liver tumors however get 100% of their blood supply from hepatic artery , so when they enhance it will be in arterial phase
In the arterial phasehypervascular tumors will enhance via the hepatic artery , when normal liver parenchyma does not yet enhances , because contrast is not yet in the portal venous system. • These hypervascular tumors will be visible as hyperdense lesions in a relatively hypodense liver
In the portal venous phasehypovascular tumors are detected when the normal liver parenchyma enhances maximally. • These hypovascular tumors will be visible as hypodense lesions in a relatively hyperdense liver.
In the equilibrium phaseat about 10 minutes after contrast injection , tumors become visible, that either : - retain their contrast ( become relatively hyperdense to the normal liver ) - wash out their contrast faster than normal liver parenchyma ( become relatively hypodense to the normal liver ).
Above: arterial phase showing hypervascular FNH • Middle: portal venous phase showing hypovascular metastases • Down: equilibrium phase showing relatively dense cholangiocarcinoma
Optimal timing Hypervascular tumors will enhance optimally at 35 seconds after contrast injection (late arterial phase)
A patient who underwent two phases of arterial imaging at 18 and 35 seconds . • In the early arterial phasewe nicely see the arteries , but we only see some irregular enhancement within the liver . • In the late arterial phase, we can clearly identify multiple tumor masses.
Portal venous phase imaging work on the opposite idea . We image the liver when it is loaded with contrast through the portal vein to detect hypovascular tumors. • The best moment to start scanning is at about 75 sec.
Hypovascular metastases seen as hypodense lesions in late portal venous phase
Starts when contrast is moving away from the liver and the liver starts to decrease in density . • This phase begins at about 3-4 minutes after contrast injection and imaging is best done at 10 minutes after contrast injection.
This phase can be valuable if you are looking for: 1- fast tumor washout in hypervascular tumors 2- retention of contrast in blood pool like in hemangioma 3- retention of contrast in fibrous tissue in capsule ( HCC )or scar tissue ( cholangiocarcinoma or FNH )
3- retention of contrast in fibrous tissue in capsule ( HCC ) or scar tissue (cholangiocarcinoma , FNH)
Hypervascular hepatic tumors • 1ry • Benign • Hemangioma • Focal nodular hyperplasia • adenoma • Malignant • HCC • Fibrolamellar HCC • 2ry • Hypervascular metastasis • Primary hypervasculrtumours • Thyroid carcinoma • Choriocarcinoma • Renal cell carcinoma • Iselet cell tumors of pancreas • Malignant pheochromocytoma • Malignant melanoma • Carcinoid tumor • 15% of cancer breast
History : A 40 year old male came with abdominal pain
Technique Triphasiccontrast enhanced CT was performed for the chest, abdomen and pelvis.
Arterial phase PV phase
Hypervascular hepatic tumors • 1ry • Benign • Hemangioma • Focal nodular hyperplasia • adenoma • Malignant • HCC • 2ry • Hypervascular metastasis • Primary hypervasculrtumours • Thyroid carcinoma • Choriocarcinoma • Renal cell carcinoma • Iselet cell tumors of pancreas • Malignant pheochromocytoma • Malignant melanoma • Carcinoid tumor • 15% of cancer breast
Primary hypervasculrtumours • Thyroid carcinoma • Choriocarcinoma • Renal cell carcinoma • Iselet cell tumors of pancreas • Malignant pheochromocytoma • Malignant melanoma • Carcinoidtumor • 15% of cancer breast
Primary hypervasculrtumours • Thyroid carcinoma • Choriocarcinoma • Renal cell carcinoma • Iselet cell tumors of pancreas • Malignant pheochromocytoma • Malignant melanoma • Carcinoid tumor • 15% of cancer breast
Primary hypervasculrtumours • Thyroid carcinoma • Choriocarcinoma • Renal cell carcinoma • Iselet cell tumors of pancreas • Malignant pheochromocytoma • Malignant melanoma • Carcinoid tumor • 15% of cancer breast
Primary hypervasculrtumours • Thyroid carcinoma • Choriocarcinoma • Renal cell carcinoma • Iselet cell tumors of pancreas • Malignant pheochromocytoma • Malignant melanoma • Carcinoid tumor • 15% of cancer breast
Location of carcinoid tumor: • Appendix …………………………. 45% • Small bowel ……………………… 35% - ilium ( 91%) .. Jejenum (7%).. Duodenum ( 2%) • Rectum …………………………….. 10% • Colon ……………………………….. 5% • Stomach ………………………….. < 3%
Diagnosis Carcinoidtumor of the stomach with hypervascular metastasis to the liver
Carcinoid tumor • Low-grade malignancy, resemble adenocarcinoma, but do not have their aggressive behaviour • Clinical presentation: • Asyptomatic ( 66%) • Abdominal pain/intestinal obstruction ( 19%) • Nausea, weight loss (16%) • Palpable mass ( 14%) • Carcinoid syndrome ( 7%)
Carcinoid syndrome: • Cause: excess serotonin level when the metabolic pathway to 5-HIAA is bypassed (a) with extensive liver metastasis (b) with 1ry pulmonary/ovarian carcinoids • Recurrent diarrhea (70%) • Right sided endocardialfibroelastosis (35%), resulting in tricuspid regurgitation and right heart failure • Desquamative skin lesions / pellagra /nausea /vomiting /fever/cutaneous flushing ….. (5%) • Prognosis: carcinoid syndrome has a higher morbidity and mortality than does the tumor itself