Download
1 / 31
310 likes | 317 Views
Prevalence and Variability of Depressive Symptoms among MESA participants Preliminary Findings. Hochang Benjamin Lee, M.D. Assistant Professor of Psychiatry and Behavioral Sciences Johns Hopkins University School of Medicine Associate Director of Research Development

E N D
Prevalence and Variability of Depressive Symptoms among MESA participantsPreliminary Findings Hochang Benjamin Lee, M.D. Assistant Professor of Psychiatry and Behavioral Sciences Johns Hopkins University School of Medicine Associate Director of Research Development Department of Psychiatry, Johns Hopkins Bayview Medical Center
Goals • Quick Review Depression-CVD relationship • Heterogeneity of “depression” and its importance in Depression-CVD relationship • Across age groups • Across race/ethnic groups • Focus on Asians and Asian-Americans • Depressive symptoms in MESA • Prevalence across race/ethnic groups • Correlates • Symptom Variability • Future directions?
What is Depression? • What is depression? • Depression: Syndrome of low mood, low self-attitude, and loss of energy (Emil Kraepelin) • Associated with disruption in neurotransmitter system (e.g. serotonergic system) • No biological marker exists. Diagnosis relies on phenotyping based on subjective reports
Diagnostic Criteria for Major Depressive Disorder according to Diagnostic and Statistical Manual-IV) • At least five of the nine symptoms below for the same two weeks or more, for most of the time almost every day, and this is a change from his/her prior level of functioning. One of the symptoms must be either (a) depressed mood, or (b) loss of interest. • 1. Depressed mood. • 2. significantly reduced level of interest or pleasure in most or all activities. • 3. A considerable loss or gain of weight (e.g., 5% or more change of weight in a month when not dieting). This may also be an increase or decrease in appetite. • 4. Difficulty falling or staying asleep (insomnia), or sleeping more than usual (hypersomnia). • 5. Behavior that is agitated or slowed down. Others should be able to observe this. • 6. Feeling fatigued, or diminished energy. • 7. Thoughts of worthlessness or extreme guilt (not about being ill). • 8. Ability to think, concentrate, or make decisions is reduced. • 9. Frequent thoughts of death or suicide (with or without a specific plan), or attempt of suicide.
Problems with phenotyping depression • Heterogeneity of depression: • Across Age • Adolescent depression • Geriatric depression • Across Gender • Depression in Men • Depression in women
Depression and CVD • One of the most replicated findings in psychiatry • Depression as a risk factor for: • New onset CVD in “CVD-free” individuals • OR: 1.64 (1.29-2.08) -Rugulies et al, 2002 • Post-MI morbidity and mortality • OR: 2.61 (1.53-4.47) -Barth et al, 2004
DEPRESSION Biological e.g., inflammatory Plaque formation CARDIOVASCULAR Behavioral smoking, diet, physical activity Obesity CONFOUNDERS Obesity Socioeconomic status Gender Race, ethnicity
Depression is a risk factor for vascular diseases (Musselman, et al, 1999, AGP)
Zung Depression Scale Barefoot et al, 1996: 1.26(1.07,1.48), US CES-D, Borowicz et al, 2002: not significant, U.S. Hospital Anxiety and Depression Scale Hermann et al, 2000: 1.21 (1.04,1.42) Germany Mayou et al, 2000: not significant, UK Depression Items Jenkinson et al, 1993: not significant, UK Other non-depression measures Ladwig et al, 1991,1994: 4.9 (1.11,21.59), Germany Denollet et al, 1996: 2.68(1.33,5.45), Belgium Denollet et al, 1998: 7.46 (1.56, 35.8), Belgium Beck Depression Inventory – Bush et al, 2001: 2.2 (1.03, 7.61), US Connery 2.31: (1.17,4.56), Canada Frasure-Smith et al, 1993,1996,1999: 4.29 (3.14,5.86), Canada Frasure-Smith et al, 1999,2000, 2002: 3.11 (1.65,6.31), Canada Irvine et al, 1999: 2.45 (1,14, 5.45), US Romanelli et al, 2002: 4.71(1.67,13.31), US Wellin et al, 2000: 3.54 (1.85,6.77), Sweden Lane et al, 2001, 2002 in UK: no difference Clinical Interview for DSM MDD Carney et al, 2003: 2.4 (1.2-4.7), U.S. Kaufmann et al, 1999: 2.34 (1.18, 4.65), U.S. Schleifer et al, 1989: not significant, U.S. How did they assess “Depression” in post-MI?
Heterogeneity of Depression: RACE/ EthnicityCross-national epidemiology of major depression and bipolar disorder. (Weissman MM, et al, JAMA, 1994) • Compared community survey data in United States, Canada, Puerto Rico, France, West Germany, Italy, Lebanon, Taiwan, Korea, and New Zealand • N= 38,000 • Diagnostic Interview Schedule – DSM III diagnosis of MDD • Similar methods in sampling and instrumentation to ensure comparability across the countries
Table Transcultural variation in the prevalence of depression: results from the Cross-National Collaborative Group (data from Weissman et al, 1996)
Lifetime and Twelve-Month Prevalence Rates of Major Depressive Episodes and Dysthymia Among Chinese Americans in Los Angeles (Takeuchi et al, AJP, 1998) • Primary assessment tool – CIDI (in English, Mandarin, or Cantonese) • 1,747 Chinese-Americans in LA county, selected with a stratified cluster sampling method • Prevalence of MDD was 6.9% (Lifetime); 3.4% (12-months) • 16.9% and 10% for U.S. adults (Kessler et al, 1994) • No association with gender and other sociodemographic variables. • What did CIDI measure (or not measure)?
Neurasthenia –”Nerve exhaustion” or “shenjing shuairuo” • DSM II had it, and DSM III dropped it. • ICD-10 Definition of Neurasthenia • Persistent and distressing complaints of increased fatigue after mental effort or persistent and distressing complaints of bodily weakness and exhaustion after minimal effort. • At least two of the following: feelings of muscular aches and pains, dizziness, tension headaches, sleep disturbance, inability to relax, irritability, dyspepsia. • Chinese Psychiatrist diagnosed Neurasthenia – one-third of their patients (Kleinman et al, 1982) • “Depression may take on more somatic yet less psychological form” • Approximates Somatization disorder in DSM IV • (prevalence 0.5 -1.0% in general U.S. adult population) -
An epidemiological study of neurasthenia in Chinese-Americans in Los Angeles.(Zheng et al, Compr Psych1997 Sep-Oct;38(5):249-59. • Goal: Prevalence of ICD-10-defined neurasthenia (NT) in Chinese-Americans • CIDI + supplemental NT module • The SCL-90-R. • Results: 12 month prevalence of NT: 6.4%. (MDD: 3.4%) • NCS rate of MDD: 10%, Somatoform disorder: 1% • Of these, 63 (56.3%) did not experience any current and lifetime DSM-III-R diagnoses, yielding a 12-month or lifetime prevalence rate of "pure" NT of 3.61%. • Compared with subjects with depression and anxiety disorders, "pure" NT cases reported significantly less SCL-90-R psychological symptoms (P < .05 or .01), but had a striking elevation in the somatization subscale score.
Summary • Many studies have demonstrated the relationship between depression and CVD. • All of the prospective studies have been from Western Countries • New Onset CVD: 9 US, 2 Europe • Post-MI Depression: 9 US, 3 Canada, 8 Europe • Few studies have examined the issue of race/ethnicity • Instrumentation seem to matter greatly (i.e. BDI over any other rating instruments) in predicting CVD mortality. • BDI relies on physical symptoms • Artificially inflated BDI due to symptoms of the illness? • Good at detecting more somatic form of depression?
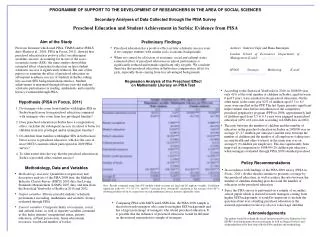
MESA Enrollment- Exam 1, 2000. • Available Data • Demographics • Socioeconomic Status • Health Behavior Measures • Extensive subclinical CVD measures • Depression Measure • Center for Epidemiologic Study – Depression (CES-D) Scale • 20 items (0-60)
Aim of Analysis • To examine and compare the prevalence and correlates of depressive symptoms (measured by the Center for Epidemiologic Studies-Depression scale) among older adults (>45 years of age) participants of MESA, both across and within race/ethnic groups. • Hypothesis: Prevalence of depression (defined by CES-D) is lower among Chinese-Americans and higher among Hispanic Americans compared to White and African-Americans.
DATA • Main Dependent variable: Responses to CES-D questionaire • Mean CES-D score • CES-D 16 or above • CES-D 22 or above • Syndromal CES-D based on an algorithm that approximates DSM III criteria for MDD • Cross-tabulations and chi-squares. • logistic regression models (race and depression) • Sociodemographic factors • health-related factors • acculturation-related factors • psychosocial factors
Baseline Mean CES-D and % CES-D score of 16 or greater in the MESA *ANOVA difference between means. **Chi-Square Test
Prevalence of CES-D score of 22 or greater and Syndromal Depression in the MESA *Chi-Square Test
CES-D score stratified by age and gender • CES-D score consistently lower above age 65 across all race/ethnic groups • CES-D score consistently higher among women than women across all race/ethnic groups
Sociodemographic factors • Female, younger age, not married, and income<30,000 were significant associated with CES-D score of 16 or higher based on logistic regression model.
Acculturation variables • Other language used, proportion of life in U.S.
Health-related variables • All of the above variables were associated with with CES-D score of 16 and above
Psychological Variables • Emotional support index, and chronic burden score were associated with CES-D score of 16 and above. • Spielberger Anxiety score was collinear
Adjusted Odds Ratios (ORs) with Confidence Intervals for Depression in Multivariate Analysis Adjusted for sociodemographic, acculturation, health-related, psychological variables. NS = not significant (P<0.05) Hispanic Americans more likely do be “depressed” and Chinese Americans less likely to be “depressed” in MESA
Being on antidepressant, CES-D 16 or above, at all six sites. White:27.3% African A: 8.1% Chinese A: 3% Hispanic A: 11.3% Being on antidepressant, CES-D 22 or above, at all six sites White: 33.6% African A:10.9% Chinese A: 4% Hispanic A: 12.8% Treatment of Depressive symptoms: MESA Study
Summary: Variability of Prevalence of Depression across race/ethnic groups • The differences in rates for major depression across race/ethnic groups suggest that cultural differences affect the expression of the disorder in MESA. • In MESA, Chinese Americans appear to be less categorized as depressed while Hispanic Americans are more likely. • Heterogeneity of depression phenotype across race/ethnicity should be considered in examining the relationship between “depression” and CVD
Thanks to Writing Group • Annette Fitzpatrick (UW) • Sherita Golden (Hopkins) • Pam Schreiner (Minnesota) • Ana Diez Roux (Michigan) • Constantine Lyketsos (Hopkins)
Correlates for CES-D =16 or above across the race/ethnic groups