Download
1 / 46
520 likes | 686 Views
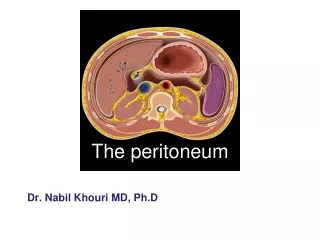
Anatomy of the peritoneum. Greek, peritonaion = stretch around The peritoneum is a large serous membrane lining the abdominal cavity. Histologically, it is composed of an outer layer of fibrous tissue (which gives strength to the membrane)

E N D
Greek, peritonaion = stretch around • The peritoneum is a large serous membrane lining the abdominal cavity. • Histologically, it is composed of an • outer layer of fibrous tissue (which gives strength to the membrane) • inner layer of mesothelial cells (which secrete a serous fluid which lubricates the surface thus allowing the free movement of the viscera )
The peritoneum is in the form of a closed sac invaginated by a number of viscera • Parietal peritoneum – outer layer-lines the walls of the abdominal and pelvic cavities • Visceral peritoneum – inner layer-covers the organs • Peritoneal cavity –the potential space between the parietal and visceral layer of peritoneum • In the male, it is a closed sac, but in the female, there is a communication with the exterior through the uterine tubes, the uterus, and the vagina
Parietal peritoneum • Embryologically, it is derived from the somatopleural layer of the lateral plate mesoderm. • Blood supply & nerve supply are the same as those of the overlying body wall • It is pain sensitive because of the somatic innervation. • It can be easily stripped as it is loosely attached to the walls by extra-peritoneal connective tissue.
Visceral peritoneum • Embryologically it is derived from the splanchno-pleural layer of the lateral plate mesoderm. • Blood supply & nerve supply are the same as those of the underlying viscera. • It is pain insensitive because of the autonomic innervation. • It is firmly adherent to the viscera & cannot be stripped; forms part & parcel of the viscera.
The relationship between viscera and peritoneum • Many organs in the abdomen are suspended by folds of peritoneum. Such organs are mobile/ intraperitoneal. The degree & direction of mobility are governed by the size & direction of peritoneal fold. • Other organs are fixed & immobile. They rest directly on the posterior abdominal wall, & may be covered by peritoneum on one side. Such organs are said to be retroperitoneal.
Peritoneal folds are given various names! • Prefix ‘mes’ or ‘meso’ (in the middle of), followed by the name of the organ • Small intestine(enteron)- mesentery • Colon- mesocolon • Large folds attached to the stomach are called omenta (omentum=cover) • Double-layered folds of peritoneum connect organs to the abdominal wall or to each other- called ligaments • Gastrosplenic ligament
Peritoneal folds • They are best understood by recapitulating the embryology of the gut • Developing gut- divisible into 3 parts foregut, midgut & hindgut • Each part has its own artery which is a ventral branch of the abdominal aorta • Coeliac- foregut, SMA- midgut, IMA-hindgut
Foregut- esophagus, stomach, upper part of duodenum (till CBD opening in D2) • Midgut- rest of duodenum, jejunum, ileum, appendix, caecum, ascending colon, right 2/3rd of transverse colon • Hindgut- left1/3rd of transverse colon, descending colon, sigmoid colon, rectum, upper part of anal canal upto pectinate line
The peritoneal cavity is divided broadly into two parts • Main larger part is known as the greater sac • Smaller part situated behind the stomach, lesser omentum & liver is known as the lesser sac • Two sacs communicate through the epiploic foramen(of Winslow)
Sex differences Male • Peritoneum is a closed sac lined by mesothelium (flattened epithelium) Female • peritoneal cavity communicates with the exterior thro the uterine tubes • the peritoneum covering the ovaries is lined by cubical epithelium • the peritoneum covering the fimbria is lined by columnar ciliated epithelium
Structures which are formed by peritoneum Omentum fold of peritoneum that extends from stomach to adjacent organs Greater omentum
Greater omentum four-layered fold of peritoneum, the anterior two layers descend from the greater curvature of stomach and superior part of duodenum and hangs down like an apron in front of coils of small intestine, and then turns upward and attaches to the transverse colon.
Lesser omentum two layered fold of peritoneum which extends from porta hepatis to lesser curvature of stomach and superior part of duodenum • Hepatogastric ligament extends from porta hepatis to lesser curvature of stomach • Hepatoduodenal ligament Extends from porta hepatis to superior part of duodenum Contains common bile duct, proper hepatic a. and hepatic portal v. Lesser omentum
Lessersac Greater sac
Omental foramen • Behind the right border of hepatoduodenal ligament • Superior-caudate lobe of liver • Inferior-superior part of duodenum • Anterior- lesser omentum ,hepatodudenal ligament • Posterior-peritoneum covering the inferior vena cava
Omental bursa /lesser sac Position-situated behind the lesser omentum and stomach Walls • Superior-peritoneum which covers the caudate lobe of liver and diaphragm • Anterior-formed by lesser omentum, peritoneum of posterior wall of stomach, and anterior two layers of greater omentum • Inferior-conjunctive area of anterior and posterior two layers of greater omentum • Posterior-formed by posterior two layers of greater omentum, transverse colon and transverse mesocolon, peritoneum covering pancreas, left kidney and suprarenal gland
Left-formed by the spleen, gastrosplenic ligamentand splenorenal ligament • Right-formed by omental foramen The Omental bursa (lesser sac) communicates with the greater sac through the omental foramen.
Mesenteries or mesocolons-two-layered fold of peritoneum that attach part of the intestines to the posterior abdominal wall
Mesenteries: result from the invagination of "intraperitoneal" organs into the sac. The mesenteries connect viscera to the posterior abdominal wall and are VERY important in that they conduct blood vessels and nerves.
Mesentery suspends the small intestine from the posterior abdominal wall • Broad and a fan-shaped • Consists of two peritoneal layers • Intestinal border-folded, 7 m long • Root of mesentery • 15 cm long • Directed obliquely from left side of L2 to in front of right sacroiliac joint
Mesoappendix • Triangular mesentery-extends from terminal part of ileum to appendix • Appendicular artery runs in free margin of the mesoappendix
Transverse mesocolona double fold of peritoneum which connects the transverse colon to the posterior abdominal wall Sigmoid mesocolon inverted V-shaped, with apex located in front of left ureter and division of common iliac artery
Ligaments -two-layered folds of peritoneum that attached the lesser mobile solid viscera to the abdominal wall Ligaments of liver • Falciform ligament of liver • Consists of double peritoneal layer • Extends from anterior abdominal wall (umbilicus) to liver • Free border of ligament site of ligamentum teres
Coronary ligament the area between upper and lower parts of the coronary ligament is the bare area of liver, this area is devoid of peritoneum and lies in contact with the diaphragm • Left and right triangular ligaments formed by right extremity of coronary ligament and left leaf of falciform ligament, respectively
Hepatogastric ligament • Hepatoduodenal ligament • Ligamentum teres hepatis
Ligaments of spleen • Gastrosplenic ligament-a double layer of peritoneum that connects the fundus of stomach to hilum of spleen. In this double layer of peritoneum are the short gastric and left gastroepiploic vessels • Splenorenal ligament-extends between the hilum of spleen and anterior aspect of left kidney. The splenic vessels lies within this ligament, as well as the tail of pancreas • Phrenicosplenic ligament • Splenocolic ligament
Ligaments of stomach • Hepatogastric ligament • Gastrosplenic ligament • Gastrophrenic ligament • Gastrocolic ligament • Gastropancreatic ligament
Folds and recesses of posterior abdominal wall • Superior duodenal fold and recess • Inferior duodenal fold and recess • Intersigmoid recess formed by the inverted V attachment of sigmoid mesocolon
Retrocecal recess in which the appendix frequently lies • Hepato-renal recess lies between the right lobe of liver, right kidney, and right colic flexure
Hepato-renal recess is the lowest part of the peritoneal cavity when the subject is supine
Folds and fossas of anterior abdominal wall • Median umbilical fold -contain the remnant of urachus (median umbilical ligaments) • Medial umbilical fold-contains remnants of the umbilical arteries (medial umbilical ligaments) • Lateral umbilical fold -contains the inferior epigastric vessels • Supravesical fossa • Medial inguinal fossa • Lateral inguinal fossa
Pouches • In male-rectovesical pouch • In female • Rectouterine pouch between rectum and uterus • Vesicouterine pouch between bladder and uterus
Peritoneal subdivisions The transverse colon and transverse mesocolon divides the greater sac into supracolic and infracolic compartments. Supracolic compartments (subphrenic space)-lies between diaphragm and transverse colon and transverse mesocolon Suprahepatic recesslies between the diaphragm and live-the falciform ligament divides it into right and left suprahepatic recesses
Left supra-hepatic recesses • left anterior supra-hepatic spaces • left posterior supra-hepatic spaces • Right supra-hepatic recesses • right anterior supra-hepatic spaces • right posterior supra-hepatic spaces • bare area of live (extra-peritoneal space)
Infra-hepatic recess lies between the liver and transverse colon and transverse mesocolon. Ligamentum teres hepatic divides it into right and left infra-hepatic recesses • Right infra-hepatic recesses (hepatorenal recess) • Left infra-hepatic recesses • left anterior infra-hepatic space • left posterior infra-hepatic space
Infra-colic compartmentlies below the transverse colon and transverse mesocolon • Right para-colic sulcus (gutter) lies lateral to the ascending colon. It communicates with the hepa-torenal recess and the pelvic cavity. It provides a route for the spread of infection between the pelvic and the upper abdominal region. • Left para-colic sulcus (gutter) lies lateral to the descending colon. It is separated from the area around the spleen by the phrenico-colic ligament, a fold of peritoneum that passes from the colic flexure to the diaphragm.
Right mesenteric sinustriangular space, lies between root of mesentery, ascending colon, right 2/3 of transverse colon and transverse mesocolon • Left mesenteric sinuslies between root of mesentery, descending colon, left 1/3 of transverse colon and transverse mesocolon, it widens below where it is continuous with the cavity of the pelvis
Functions of the peritoneum Movements of viscera • Slippery surface for free movements of abdominal viscera • Permits peristalsis of stomach, intestine • Abdominal movements during respiration • Periodic changes in the capacity of hollow viscera assoc with their filling & evacuation
Functions of the peritoneum Protection of viscera • Contains phagocytic cells which guard against infection • Lymphocytes provide both cellular & humoral immunological defense mechanisms • Greater omentum has the power to move towards sites of infection & to seal them, thus preventing spread of infection ‘policeman of the abdomen’
Functions of the peritoneum Absorption • The mesothelium acts as a semi-permeable membrane across which fluids & small molecules of various solutes can pass. Thus, it can absorb fluid effusions from the peritoneal cavity • Water & crystalloids are absorbed directly into the blood capillaries, whereas colloids pass into lymphatics with the aid of phagocytes • The greater absorptive power of the sub-phrenic area is due to its larger surface area & becoz respiratory movements aid absorption
Functions of the peritoneum Dialysis • Metabolites like urea can be removed from the blood by artificially circulating fluid through the peritoneal cavity – peritoneal dialysis Therapeutically, considerable volumes of fluid can be administered through the peritoneal cavity
Functions of the peritoneum Healing power & adhesions • The mesothelial cells can transform themselves into fibroblasts, which promote healing of wounds. • They may also form adhesions causing obstruction in hollow organs Storage of fat • Capable of storing large amounts of fat