Download
1 / 39
620 likes | 1.49k Views
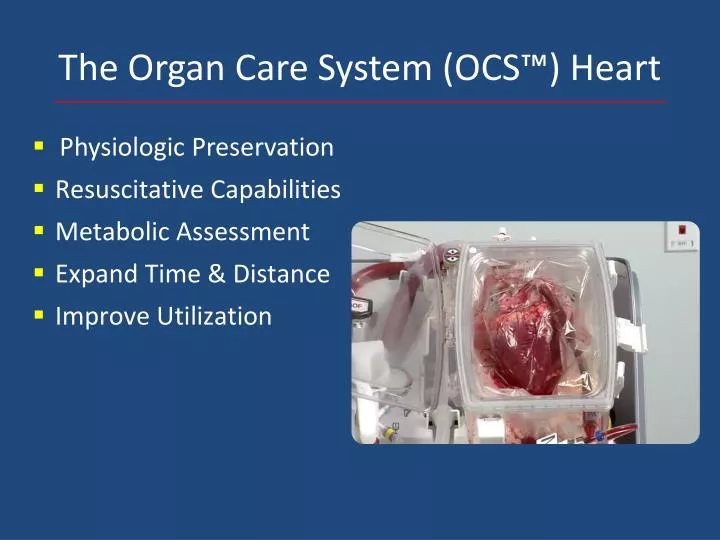
The Organ Care System (OCS™) Heart. Physiologic Preservation Resuscitative Capabilities Metabolic Assessment Expand Time & Distance Improve Utilization . Ex-Vivo Perfusion of Hearts With The TransMedics Device – US Experience. PROCEED II Trial Overview.

E N D
The Organ Care System (OCS™) Heart • Physiologic Preservation • Resuscitative Capabilities • Metabolic Assessment • Expand Time & Distance • Improve Utilization
Ex-Vivo Perfusion of Hearts With The TransMedics Device – US Experience
PROCEED II Trial Overview Goals: FDA Clearance of OCS Technology in US for Donor Heart Preservation Design: Prospective, Randomized (1:1), Multi-center, Non-Inferiority Trial Comparing the Safety & Efficacy of OCS to Cold Storage of Donor Hearts Primary Endpoint: 30-Day Patient & Graft Survival Success Criteria: OCS group is statistically not inferior to SOC • Secondary Endpoints: • Incidence of Cardiac-related SAEs • Incidence of Bx. Proven ISHLT Grade 2R or 3R Rejection • Incidence of Clinically Symptomatic Rejection • ICU Time
PROCEED II Overall Enrollment Status 130 Total Randomized 126 Transplanted 4 Turned Down Based on OCS Lactate This Interim Report on 116 Patients Transplanted and Met the 30-day Endpoint
OCS Group Cross Clamp Time (n=55) Total Time (mean ± SD) = 325 ± 79 min RECIPIENT Range = 149 – 543 min
OCS Perfusion Parameters (n=55) Mean ± SE OCS CF OCS HR OCS AOP
OCS Perfusion – Lactate Levels (n=55) Mean ± SE
Cases Evaluated On OCS and Turned Down Based OCS Lactate (n=4)
OCS Perfusion Parameter & Lactate Trend (n=4) Mean ± SE Mean ± SE
OCS Identified Hidden Donor Pathology (n=4) Hypertrophy Infarction AO Valve Incompetence
Conclusion • The OCS use has shown to be as safe and effective as the current standard of care • OCS Lactate trend continues to be a sensitive indicator for donor heart condition
Next Steps • OCS Heart EXPAND Trial focusing on extended criteria donor hearts to: • Evaluate the impact of OCS on improving the utilization of donor hearts to increase the number of heart transplants
Ex Vivo Lung Perfusion • Platform to perfuse the donor lungs in an ex vivo circuit, with the goals of assessment and repair. • Static EVLP • Portable EVLP
Static EVLP Vs. Portable OCS Lung • Ischemic injury • No recruitment • No assessment • Delayed benefits • Resource intensive • Delayed clinical decision making • Reduction of ischemia • Immediate & sustained recruitment • Continuous monitoring & assessment of function • Existing resources and Streamlined decision making process
Roman, MA; et. al., Ex Vivo Lung Perfusion. Transplantation 96(6) 509–518
Static EVLP Protocol • Acellular (steen solution) • Initial flow rate of 50-100cc/min to 40%-100% cardiac output (maintain PA < 15-20 mmHg) • Ventilate when temp >32°F, 7cc/kg @ 7 per min, FIO2 (.21-.5) • Assessment Parameters (1-4 hrs) PaO2/FIO2 > 350, PVR, dynamic compliance, and peak airway pressure ≥ 85% of baseline
Static EVLP • 23 high risk donor lungs were placed on EVLP for 4 hours • PaO2 increased from 335 mmHg in the donor to 443 mmHg at 4 hrs of EVLP • 20 of 23 donor lungs were transplanted with PGD III at 72° of 15% and 1 month survival of 90%, similar to historical cohort. Cypel M et. al., Normothermic Ex Vivo Lung Perfusion in Clinical Lung Transplantation, N Engl J Med 2011; 364: 15: 1431-1440.
The INSPIRE Trial Background • Prospective randomized pivotal international trial for lung preservation for transplantation; • comparing portable ex-vivo cellular perfusion to static cold preservation to evaluate the impact on post transplant outcomes in routine lung transplantation • Registered NCT01630434
Trial Endpoint • Primary Endpoint: Composite patient survival at 30 days and incidence of PGD 3 • Secondary Endpoints: • Incidence of PGD 3 • Incidence of PGD 2+3 • Patient survival • Graft survival
OCS Lung Oxygenation Capacity • Pulmonary flow =2-2.5 L/min • OCS monitor the SvO2/SaO2 • ABG at ~120 sec. to calculate PaO2/FiO2 ratio
Incidence of Post-Transplant Primary Graft Dysfunction (PGD) Grade 3 P=0.003 N=59 77
Composite Primary Endpoint Survival & PGD 3 T0-T72 Hours p=0.011 N=59
Conclusions • OCS is safe for preservation of standard donor lungs • To-date interim INSPIRE results demonstrate: • reduction of PGD3 incidence • difference of the composite endpoint • positive trend towards improved survival and patient outcomes • EXPAND pivotal international trial is designed to build prospective evidence to support increasing –extended criteria- donor lung utilization
US Lung Waiting List Dynamics Source: http://optn.transplant.hrsa.gov
Donor’s condition • Improve donor organ • Understand the local Transplant Centers’ needs • Collaborate
Final Remarks • Ex vivo thoracic organ perfusion • Will continue to evolve (as a technology) • Improve the donor organ • Allow assessment of the donor/expand the donor pool • Provide a platform to repair/enhance the donor organ