Download
1 / 28
320 likes | 538 Views
Le point sur Oncotype et les équivalents SFCP 19 septembre 2008. Dominique Spaëth Centre d’Oncologie de Gentilly - NANCY. Prescrivons nous un traitement adapté ? Adjuvant on line. Prognosis Classifier for Breast Cancer based on Genomic Profiling. Columns: tumor samples.

E N D
Le point sur Oncotype et les équivalentsSFCP 19 septembre 2008 Dominique Spaëth Centre d’Oncologie de Gentilly - NANCY
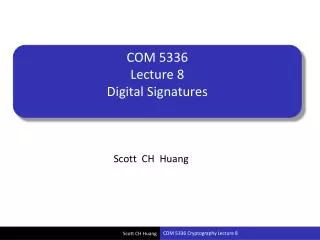
Prognosis Classifier for Breast Cancer based on Genomic Profiling Columns: tumor samples Rows: 70 significant prognosis genes Good signature threshold Poor signature Threshold set with 10% false negatives 91% sensitivity; 73% specificity Metastases: white = + Van ‘t Veer et al Nature 415, p530-536, 2002
Comparison between genomic and multivariable clinical predictive models M Buyse et al, J Natl Cancer Inst 98:1183, 2006 (These results are only applicable to node negative patients)
64% 36% 33% 67% High clinicalrisk Lowclinicalrisk Low gene sign. risk Low gene signature. risk High gene sign. risk High gene signature risk 70-gene signature (Age<55, T<5cm, N0, DMS 5yrs) Discordance rates clinical vs gene signature SABS 2004, Dr Martine Piccart-Gephart JBI, Brussels
Agendia Mammaprint 70-Gene Prognostic Signature Assay C’est déjà du concret ! Genomic Health Oncotype Dx 21-Gene Recurrence Score Assay Time’s Best Invention of the Year, 2007
Development and Validation of a 21-Gene Assay for N–, ER+, Tam+ Patients YEAR Develop real-time RT-PCR method for paraffin block 2001 Select candidate genes (250 genes) 2002 Model building studies (N = 447, including 233 from NSABP B-20) 2002 Commit to a single 21-gene assay 2003 Validation studies in NSABP B-14 and Kaiser Permanente 2003 Paik et al. N Engl J Med. 2004;351:2817-2826.
Oncotype DX® 21-Gene Recurrence Score (RS) Assay 16 Cancer and 5 Reference Genes From 3 Studies PROLIFERATION Ki-67 STK15 Survivin Cyclin B1 MYBL2 ESTROGEN ER PR Bcl2 SCUBE2 GSTM1 BAG1 INVASION Stromelysin 3 Cathepsin L2 CD68 REFERENCE Beta-actin GAPDH RPLPO GUS TFRC HER2 GRB7 HER2 Paik et al. N Engl J Med. 2004;351:2817-2826.
Intermed. risk 27.0% Low risk 51.0% High risk 22.0% A Multigene Assay to Predict Recurrence of Tamoxifen-Treated, Node-Negative Breast Cancer Results:Population distribution by Oncotype DX risk group Paik .S. et al. N Engl J Med 2004;351:2817-26
Distant Recurrence-Free Survival (%) 100 80 60 DRFS (%) 40 All patients Low Risk (RS < 18) Intermediate Risk (RS 18 - 30) 20 High Risk (RS 31) 0 0 2 4 6 8 10 12 14 16 Years 93% P < 0.00001 69% Paik .S. et al. N Engl J Med 2004;351:2817-26
Oncotype DX® Clinical Validation: RS as Continuous Predictor My RS is 30. What is the chance of recurrence within 10 years? 95% CI
Bénéfice du Tamoxifène et Oncotype DX® NSABP B-14 Tam Benefit Study in N–, ER+ Patients Design Objective: Determine whether the 21-gene RS assay provides information on: 1) Prognosis (likelihood of recurrence) 2) Response to tamoxifen (change in likelihood of recurrence with tamoxifen) 3) Both Placebo-Eligible Randomized Tam-Eligible Paik et al. ASCO 2004. Abstract #510.
NSABP B-14 Benefice du Tamoxifène All Patients (N = 645) 1.0 0.9 0.8 0.7 0.6 DRFS 0.5 0.4 0.3 0.2 Placebo 0.1 Tamoxifen 0.0 12 0 2 4 6 8 10 14 16 Years Paik et al. ASCO 2004. Abstract #510.
1.0 1.0 1.0 0.8 0.8 0.8 0.6 0.6 0.6 DRFS DRFS DRFS 0.4 0.4 0.4 0.2 0.2 0.2 Placebo Placebo Placebo Tamoxifen Tamoxifen Tamoxifen 0.0 0.0 0.0 12 12 12 0 0 0 2 2 2 4 4 4 6 6 6 8 8 8 10 10 10 14 14 14 16 16 16 Years Years Years NSABP B-14 Benefice du Tamoxifène Low Risk (RS<18) Int Risk (RS 18-30) N 171 142 N 85 69 High Risk (RS≥31)1 N 99 79 Paik et al. ASCO 2004. Abstract #510.
Design Objective: Determine the magnitude of the chemo benefit as a function of the 21-gene RS assay Bénéfice de la chimiothérapie et Oncotype DX® NSABP B-20 Chemo Benefit Study in N–, ER+ Pts Tam + MF Randomized Tam + CMF Tam Paik et al. J Clin Oncol. 2006;24:3726-3734.
NSABP B-20 Résultats Tam vs Tam + Chemo – All 651 Patients 1.0 0.9 4.4% absolute benefit from tam + chemo 0.8 0.7 0.6 DRFS 0.5 0.4 0.3 N Events 424 33 227 31 0.2 All Patients Tam + Chemo P = 0.02 0.1 Tam 0.0 2 4 6 8 10 12 0 Years Paik et al. J Clin Oncol. 2006.
High Risk Patients (RS>31) N Events TAM + Chemo 117 13 TAM 47 18 Low Risk Patients (RS<18) N Events TAM + Chemo 218 8 TAM 135 4 Int Risk Patients (RS 18-31) N Events TAM + Chemo 89 9TAM 45 4 NSABP B-20 Résultats Low RS Int RS p = 0.39 p = 0.61 28% absolute benefit from tam + chemo High RS p < 0.001 Paik et al. J Clin Oncol. 2006.
B-20 Results: Absolute % Increase in DRFS at 10 Years n = 353 Low RS <18 n = 134 Int RS 18-30 n = 164 High RS ≥31 0 10% 20% 30% 40% % Increase in DRFS at 10 Yrs (mean ± SE) Paik et al. J Clin Oncol. 2006.
Standardized Quantitative Oncotype DX Assay Recurrence Score in N-, ER+ patients • Lower RS’s • Lower likelihood of recurrence • Greater magnitude of TAM benefit • Minimal, if any, chemotherapy benefit • Higher RS’s • Greater likelihood of recurrence • Lower magnitude of TAM benefit • Clear chemotherapy benefit 1) Paik et al NEJM 2004, 2) Habel et al Breast Cancer Research 2006 3) Paik et al JCO 2006, 4) Gianni et al JCO 2005
Oncotype DX®en pratique • Oncotype DX disponible depuis janvier 2004 • Genomic Health Californie • Envoyer un bloc inclus en paraffine de tumeur ou 6 lames via FedEx avec le kit Oncotype DX™ Specimen • réponse: +/- 10 jours • USA : pris en charge • Coût 3600 US $ • France • CB obligatoire ! • Délicat +++
Prove clinical utility Independent validation of accuracy Discovery Marker optimization Clinical development stages of genomic diagnostic tests for breast cancer Current evidence ends here Phase II Phase III Phase I 95% confidence interval PROGNOSTIC TESTS 70-gene prognostic signature 21-gene recurrence score 76-gene prognostic signature “molecular classification” PREDICTIVE TESTS 44-gene Tamoxifen predictor 57-gene EC predictor 92-gene Docetaxel predictor 85-gene Docetaxel predictor 30-gene Taxol/FAC predictor 70-gene MammaPrint 21-gene Oncotype DX MINDACT Trial PACT Trial 76-gene VDX2 array ? MDACC 2003-0321
TAILORx TrialAssigning IndividuaLizedOptionsforTreatment (Rx) • ECOG, SWOG, NCCTG, CALGB, NCIC, ACOSOG, and NSABP • Promoteur NCI Node-Neg, ER-Pos Breast Cancer Register Specimen banking Oncotype DX® Assay RS 11-25 Randomize Hormone Rx vs Chemotherapy + Hormone Rx RS <10 Hormone Therapy Registry RS >25 Chemotherapy + Hormone Rx Primary study group
MINDACT Design (Microarray in Node-Negative Disease May Avoid Chemotherapy Trial) Evaluate clinico-pathological risk (Adjuvant!) AND 70-gene signature risk 32% N=780 13% N=330055% Discordant cases Clin-Path HIGH risk 70-gene LOW risk Clin-Path LOW risk 70-gene HIGH risk Clinical pathological AND 70-gene signatureHIGH risk Clinical pathological AND 70-gene signatureLOW risk n=1920 Use Clin-Path risk to decide on adjuvant chemotherapy or not Use 70-gene risk to decide on adjuvant chemotherapy or not chemotherapy No chemotherapy R All hormone responsive patients receive endocrine therapy Buyse M et al, JNCI 2006
ASCO 2007 Updated Recommendationsfor Breast Cancer Tumor Markers • CA 15-3 and CA 27.29 • Carcinoembryonic Antigen (CEA) • Estrogen receptors and Progesterone receptors (ER and PgR) • DNA flow cytometry-based proliferation markers • Immunohistochemically-based markers of proliferation NEW! • HER2 • p53 as a marker for breast cancer • Cathepsin D • Urokinase plasminogen activator (uPA) and plasminogen activator inhibitor 1 (PAI-1) NEW! • Cyclin E NEW! • Proteomic Analysis NEW! • Multiparameter gene expression analysis NEW! • Bone marrow micrometastases NEW! • Circulating Tumor Cells NEW!
Multiparameter Gene ExpressionAnalysis for Breast Cancer • Oncotype DX™ can be used to determine prognosis in newly diagnosed patients with node-negative, estrogen-receptor positive breast cancer who will receive tamoxifen. Indications: – To predict risk of recurrence in patients considering treatment with tamoxifen – To identify patients who are predicted to obtain the most therapeutic benefit from adjuvant tamoxifen and may not require adjuvant chemotherapy – Patients with high recurrence scores appear to achieve relatively more benefit from adjuvant chemotherapy (specifically CMF) than from tamoxifen • Conclusions may not be generalizable to hormonal therapies other than tamoxifen, or to other chemotherapy regimens. • Several other multi-parameter assays have been reported and a few are commercially available, including Mammaprint and the Rotterdam Signature. However, the Committee felt that the precise clinical utility and appropriate application for these other assays were insufficiently defined to recommend their use.
Conclusions • Les débuts d’une médecine prédictive individualisée pour le cancer du sein • Aussi tests prédictifs de sensibilité au Tt • Oncotype pour N- RH+ • Moins de sur-traitement et plus d’économies • Si vous avez des doutes, ou pour faire bénéficier gratis vos patientes … participez à MINDACT !!!!