Download
1 / 88
1.76k likes | 6.01k Views
Extraocular Muscles. A Little Pull Can Do wonders!. Structure of the Extraocular Muscles. Extraocular muscle has a denser blood supply and a finer connective tissue muscle sheath that contains more elastic fibers than typical skeletal muscle

E N D
Extraocular Muscles A Little Pull Can Do wonders!
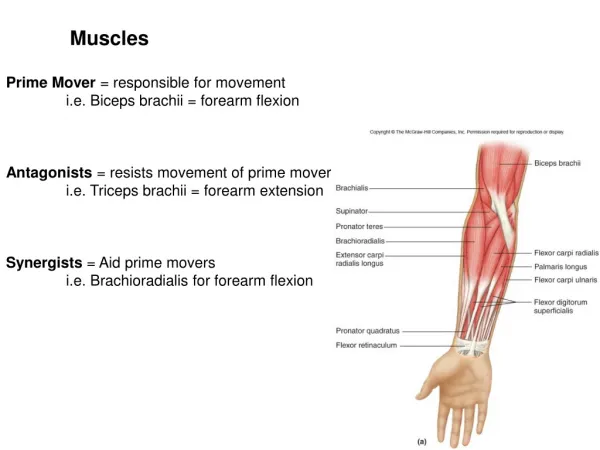
Structure of the Extraocular Muscles • Extraocular muscle has a denser blood supply and a finer connective tissue muscle sheath that contains more elastic fibers than typical skeletal muscle • Compared to skeletal muscle elsewhere, an extraocular motor unit has fewer muscle fibers, so their innervation ratio is higher—each axon innervates only 3 to 10 fibers • This high innervation ratio gives the EOMs precise fine motor control and the ability to move the eye quickly and accurately • The fibers nearer the surface of an EOM are of smaller diameter than those in the middle of the muscle • The fibers range from typical twitch fibers to typical slow fibers, and all fibers are active to some extent in all forms of movement and muscle tonus
Structure of the Extraocular Muscles 2 • Some of the larger diameter twitch fibers are individually innervated • Extraocular muscles are among the fastest and most fatigue resistant striated muscles • Afferent proprioceptive information is thought to be signaled by a receptor that is unique to extraocular muscle, the myotendinous cylinder (palisade ending) • Muscle spindles and Golgi tendon organs have also been indentified in human EOM, but it is not known whether these structures provide any useful proprioceptive information
Fick’s Axes • All eye movements can be describes as a rotation around one or more axes--Fick assumed that these axes divided the globe into quadrants and intersect at the center of rotation, a fixed unmoving point at about the geometric center of the eyeball • It is assumed that the center of rotation is located 13.5 mm behind the anterior corneal surface—more posterior in myopes and more anterior in hyperopes • The X-axis is the horizontal or transverse axis and runs from nasal to temporal • The Y-axis is the sagittal axis running through the anterior and posterior poles of the eye • The z-axis is the vertical axis and runs superior to inferior • The anterior pole of the globe is the reference point used to describe any eye movements
Ductions • Movements involving just one eye are called ductions • Rotations around the vertical axis move the anterior pole medially—adduction—or laterally—abduction • Rotations around the horizontal axis move the anterior pole of the globe up—elevation (supraduction)—or down—depression (infraduction) • Torsions or cyclorotations are rotations around the Y-axis (sagittal axis) and are described relative to a point at the 12-o’clock position on the superior limbus • Intorsion (incyclorotation) is the rotation of that point nasally, and extorsion (excyclorotation) is the rotation of that point temporally
Ductions 2 • Torsional movements are thought to occur to compensate for head tilt—with a 30 degree head tilt, the ispsilateral eye (the one on the side to which the head is tilted) intorts about 7 degrees, and the contralateral eye extorts about 8 degrees • Some investigators believe that true torsion occurs only in pathologic conditions, but others have measured torsion in normal eye movements and with head tilt
Vergences and Versions • Vergences and versions are movements of both eyes and differ in the relative direction of the two eyes’ movements • In vergence movements the two eyes move in opposite left-right directions—these are called disjunctive movements • In convergence each eye is adducted (moved toward the midline), and in divergence each eye is abducted (moved away from the midline) • Versions are conjugate movements and occur when the two eyes move in the same direction • Dextroversion is right gaze—levoversion is left gaze • Supraversion is upward gaze (both eyes elevated)—infraversion is downward gaze (both eyes depressed)
Positions of Gaze • The primary position of gaze is that position of the eye with the head erect, the eye located at the intersection of the sagittal plane of the head and the horizontal plane passing through the centers of rotation of both eyes, and the eye focused for infinity • In the strict definition, primary position of gaze represents the unique position of the eye from which horizontal and vertical ocular positions can be reached without a rotation of the eye around its line of sight (y-axis) • Secondary positions of gaze are rotations around either the vertical axis or the horizontal axis; tertiary positions are rotations around both the vertical and the horizontal axes
Origin of the Rectus Muscles • The four rectus muscle take their origin from the common tendinous ring (annulus of Zinn)—an oval band of connective tissue positioned at the orbital apex anterior to the optic foramen and the superior orbital fissure • The upper and lower parts are thickened bands and are called the upper and lower tendons or limbs • The medial and lateral rectus take their origins from both the upper and lower tendons, and the superior rectus originates from the upper limb, and the inferior rectus originates from the lower limb
Origin of the Rectus Muscles 2 • The medial rectus and superior rectus also attach to the dural sheath of the optic nerve • The area enclosed by the tendinous ring is called the oculomotor foramen, and a number of nerves and a few blood vessels pass through it, having entered the orbit through the optic canal, or the superior orbital fissure • The optic nerve and ophthalmic artery enter the oculomotor foramen through the optic canal—the superior and inferior divisions of the oculomotor nerve, the abducens nerve, and the nasociliary nerve enter the oculomotor foramen from the superior orbital fissure
Retrobulbar Neuritis • Retrobulbar neuritis is an inflammation affecting the sheaths of the optic nerve—loss ofvision is a cardinal symptom of retrobulbar neuritis • Generally there are no observable fundus changes, but pain with extreme eye movement can be one of the early presenting signs • The optic nerve sheath is supplied with a dense sensory nerve network and due to the connection between the dural and muscle sheaths, eye movement can elicit pain due to stretching of the optic nerve sheath
Origin of the Rectus Muscles 3 • All these nerves and vessels lie within the muscle cone, the area enclosed by the four rectus muscle and any connective tissue joining them—the motor nerve to each rectus muscle enters the inner surface of the muscle (the one lying within the muscle cone) • The trochlear, lacrimal and frontal nerves and the superior ophthalmic vein lie above the ring, and the inferior ophthalmic vein lies below it—outside the muscle cone
Spiral of Tillaux • The four rectus muscles insert into the globe anterior to the equator—a line connecting these insertions forms a spiral, the spiral of Tillaux • The spiral starts with the medial rectus insertion, the insertion closest to the limbus, proceeds to the inferior rectus, the lateral rectus, and, finally, to the superior rectus, the insertion farthest from the limbus • A recent study showed that although the absolute distances involved may vary considerably, the spiral of Tillaux is always observed • The muscle tendons pierce Tenon’s capsule and merge with the scleral fibers—a sleeve of capsule covers the tendon for a short distance, and the muscle can slide freely within this sleeve • Connective tissue runs from the four insertions, joining them to one another
Medial Rectus Muscle • The medial rectus (MR) is the largest extraocular muscle, its size probably due to its high usage in convergence • It takes origin from the upper and lower part of the common ring and from the sheath of the optic nerve • The medial rectus parallels the medial orbital wall until it passes through a connective tissue pulley just posterior to the equator of the globe—from this point it follows the curve of the globe to its insertion • The insertion of the MR is about 5.5 mm from the limbus, and the tendon is about 3.7 mm long • The insertion is positioned vertically so that the horizontal plane of the eye about bisects it
Medial Rectus Muscle 2 • The superior oblique muscle, ophthalmic artery, and nasociliary nerve lie above it • Fascial expansions from the muscle sheath run to the medial wall of the orbit and form the well-developed medial check ligament • The medial rectus is innervated by the inferior division of cranial nerve III, the oculomotor nerve, which enters the muscle on its lateral surface
Lateral Rectus • The lateral rectus (LR) has its origin on both limbs of the common tendinous ring and the spina recti lateralis (on the sphenoidal superior orbital fissure) • The lateral rectus runs along the lateral wall of the orbit until it passes through a connective tissue pulley just posterior to the equator of the globe—from this point forward, it follows the curve of the globe to its insertion • The insertion runs parallel to that of the medial rectus and is about 6.9 mm from the limbus • The lacrimal artery and nerve run along the superior border of the lateral rectus muscle
Lateral Rectus 2 • The ciliary ganglion, the abducens nerve, and the ophthalmic artery lie medial to the lateral rectus, between it and the optic nerve • Fascial expansions from the muscle sheath attach it to the lateral orbital tubercle and form the lateral check ligament • The lateral rectus is innervated by cranial nerve VI, the abducens nerve, which enters on the medial side of the muscle
Superior Rectus Muscle • The superior rectus (SR) takes origin from the upper part of the common tendinous ring and the sheath of the optic nerve • The muscle runs forward under the levator—the sheaths of these two are connected, which coordinates eye and eyelid movement • Another band of this connective tissue connects the SR to the superior conjunctival fornix • This muscle runs along the roof until it passes through a connective tissue pulley just posterior to the equator of the globe and afterward it follows the curve of the globe to its insertion
Superior Rectus 2 • The insertion of the SR is about 7.7 mm from the limbus and is curved slightly, with the convex side forward—the insertion is on a slight angle with the nasal side closer to the limbus than the temporal • The tendon length is about 5.8 mm • A line drawn from the origin to the insertion makes an angle of about 23 degrees with the sagittal axis • The frontal nerve runs above the SR and levator, and the nasociliary and the ophthalmic artery run below • The tendon of insertion for the superior oblique runs below the anterior part of the SR’s insertion • The superior rectus is innervated by the superior division of the oculomotor nerve, which enters the muscle on its inferior face—branches either run through or around the SR to innervate the levator
Inferior Rectus Muscle • The inferior rectus (IR) has its origin on the lower limb of the common tendinous ring—its insertion is about 6.5 mm from the limbus in an arc, convex side forward, with the nasal side closer to the limbus • The tendon length is about 5.5 mm • The IR parallels the SR, making an angle of about 23 degrees with the sagittal axis • The IR parallels the floor until a connective tissue pulley just posterior to the equator of the eye, after which it follows the curve of the globe to an insertion that parallels that of the SR • Below the IR is the floor of the orbit and above it is the inferior division of the oculomotor nerve
Inferior Rectus Muscle 2 • Anteriorly, the inferior oblique muscle comes between the inferior rectus and the orbital floor—the sheaths of these two muscles contribute to the suspensory ligament ofLockwood • The capsulopalpebral fascia, an anterior extension from the sheath of the inferior rectus muscle and the suspensory ligament, inserts into the inferior edge of the tarsal plate of the lower eyelid, allowing coordination of eye movements and lower lid movements during downward gaze • The inferior rectus is innervated by the inferior division of cranial nerve III, the oculomotor, which enters the muscle on its superior surface
Superior Oblique Muscle • The superior oblique (SO) originates from the lesser wing of the sphenoid (not from the annulus of Zinn), medial to the optic canal near the frontoethmoidal suture • The muscle runs forward, turns to tendon, and passes through the trochlea, a U-shaped pulley, in the upper inner corner of the orbit • This muscle turns to tendon about 1 cm posterior to the trochlea • The SO is the longest and thinnest extraocular muscle, largely due to its long (2.5 cm) tendon of insertion
Superior Oblique Muscle 2 • The trochlea represents the physiologic or effective origin of the muscle—that is, the line of pull of the muscle is along a line connecting this point to the point of insertion at the eyeball—this line makes an angle of 55 degrees with the visual axis • The SO lies above the medial rectus, with the nasociliary nerve and the ophthalmic artery lying between them • The superior oblique is innervated by the trochlear nerver, cranial nerve IV, which enters the posterior part of the muscle
Inferior Oblique Muscle • The inferior oblique (IO) originates on the floor of the orbit, from the maxillary bone just posterior to the inferior medial orbital rim and lateral to the nasolacrimal canal • The inferior oblique is the only extraocular muscle to originate from the front of the orbit • The muscle runs from the anterior medial corner of the orbit to insert on the lateral side of the globe—it about parallels the tendon of insertion of the SO
Inferior Oblique 2 • The insertion of the IO is on the posterior portion of the globe on the lateral side, mostly inferior, lying just outer to the macular area—the insertion is a downward concave curve • The IO makes an angle of about 51 degrees with the visual axis • Above the IO are the inferior rectus and the globe, and beneath lies the orbital floor • The IO is innervated by the inferior division of the oculomotor nerve, which enters the upper surface of the muscle
EOMs & Orbital Connective Tissue Structures • There are two layers of EOM muscle fibers: • The inner global layer is next to the globe and has a variety of fiber diameters and its fibers extend the full length of the muscle—the global layer inserts into the sclera and causes movement of the eyeball • The outer orbital layer is next to the orbital walls and consists of smaller diameter fibers, and is more vascularized than the global layer—the orbital layer inserts into the connective tissue muscle pulleys and can influence the rotational axis of the muscle • Connective tissue sleeves or pulleys couple the EOMs to the orbital walls and Tenon’s capsule
EOMs & Orbital Connective Tissue Structures 2 • Smooth muscle bundles attach the pulleys to the periorbita of the orbital wall and may assist in the coordination of binocular movements • This smooth muscle is innervated by both the sympathetic and parasympathetic system, perhaps representing both excitation and inhibition • The smooth muscle either regulates the stiffness of the pulleys or moves the pulleys to alter the direction of pull of the associated EOM—muscle sideslip may be reduced, and the effective direction of pull altered • Pulley displacement can mimic muscle dysfunction • The pulley of the medial rectus is the best developed
EOM & Orbital Connective Tissue Structures 3 • Dense connective tissue septa run between the extraocular muscle sheaths and the orbital bones and contribute to the framework supporting the eyeball within the orbit • The horizontal rectus muscles are anchored to the periorbita by their check ligaments • The medial check ligament is attached to the medial orbital wall at the posterior lacrimal crest, and the lateral check ligament is attached to the lateral orbital tubercle of the zygomatic bone—the medial check ligament is much better developed
EOM & Orbital Connective Tissue Structures 4 • These ligaments have long been thought to act to restrict the movement of the globe, i.e., in abduction the medial check ligament stops globe movement when extension of the MR begins to exert pull on the ligament • Intermuscular septa include those connecting: 1) LR, IR, and MR; 2) MR and SR; 3) LR and SR; 4) MR to SO and to orbital roof and floor; 5) MR to periorbita of ethmoid; 6) SO to frontoethmoid angle; 7) IR to orbital floor; 8) LR to lateral wall; 9) levator to periorbita, and 10) SO to orbital roof • These attachments between muscle and bone helps stabilize the muscle path and limit eye movement
Isolated Agonist Model • This model is based on analyzing the action of each muscle alone when it contracts, when it is the agonist • The model is the basis of the clinical evaluation of extraocular muscle function and is used to describe the movement of the eyeball around the axes that occurs with contraction of each muscle • However, it is important to keep in mind that during any eye movement, all six EOMs are in some state of contraction or relaxation, and that it is artificial to consider eye movement as if only one muscle contracts—in all these descriptions the eye begins in primary position
Horizontal Rectus Muscles • The horizontal recti muscle lies parallel to the sagittal axis and perpendicular to the vertical axis, so they have only one action when the eye is in the primary position of gaze • The MR has only one action—rotation around the vertical axis in a nasal direction, adduction • The LR has only one action—rotation around the vertical axis in a temporal direction, abduction
Vertical Rectus Muscles • The action of the SR is more complicated that that of the MR and LR because its line of action makes an angle with each of the axes of the eye • The primary actionof the SR is elevation, because its line of action is above the horizontal axis • The muscle’s line of action is lateral to the vertical axis (and anterior to the center of rotation), so movement around this axis causes adduction • The muscle’s line of action and oblique insertion on the superior surface of the globe also causes intorsion • This adduction and intorsion are secondary actions
Vertical Rectus Muscles 2 • The primary actionof the inferior rectus is depression, because its line of action is below the horizontal axis, and secondary actions are adduction, and extorsion
Oblique Muscles • The primary actionof the superior oblique is intorsion, because of its oblique line of action (from the trochlea to the midpoint of its tendinous insertion) it rotates the globe around its anterior posterior axis • The SO’s secondary actions are depression and abduction • The primary action of the inferior oblique is extorsion, because due to its line of action, the most rotation occurs around the anterior posterior axis • Secondary actions are elevation and abduction
Movements from Secondary Positions • As the position of the eye changes the contraction of a given muscle has a different effect than when the eye is in the primary position—this is because, with movement, the relationship between the muscle’s line of action changes relative to the axes of the eye • For example, if the eye is depressed, contraction of the horizontal rectus muscles no longer causes only adduction or abduction, but also causes a slight depression of its own
Vertical Rectus Muscles • When the eye is abducted 23 degrees from the primary position, the vertical rectus muscles’ line of action parallels the eye’s sagittal axis and is perpendicular to the horizontal axis, and they will cause only vertical movement • In this position, the superior rectus will cause pure elevation, and the inferior rectus will cause pure depression • With adduction of about 67 degrees, the line of action of the vertical rectus muscle is at a right angle with the eye’s sagittal axis, and the vertical rectus muscles will not cause any elevation or depression of the eye