Download
1 / 39
390 likes | 696 Views
OVERVIEW OF NEONATAL SURGERY. ANNE ASPIN 2010. Gastroschisis. Defect lies to right of umbilicus Central abdominal wall defect No sac. Embryology. 6 TH Week intestine grows rapidly Rotates and inverts by 10 th week Liver, bladder, stomach

E N D
OVERVIEW OF NEONATAL SURGERY ANNE ASPIN 2010
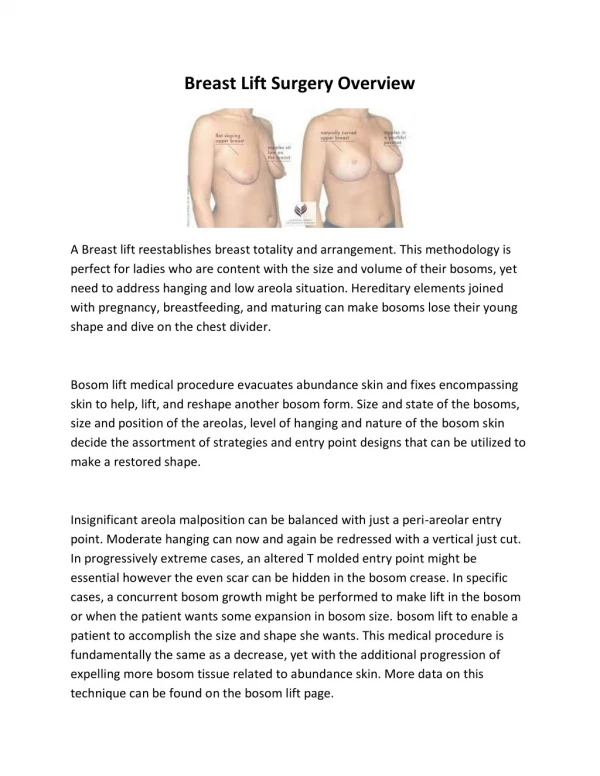
Gastroschisis • Defect lies to right of umbilicus • Central abdominal wall defect • No sac
Embryology • 6TH Week intestine grows rapidly • Rotates and inverts by 10th week • Liver, bladder, stomach • Can be caused by vascular accident.
Incidence • Omphalocele 1 :4000 • Gastroschisis 1:6000 – 10,000 • Increasing over last 30 years • Common in young mums, <20yrs.
Associated anomalies • Gastro-intestinal tract, atresia,stenosis • Duplication cysts.
Feeding problems • Gastro-oesophageal reflux • Vomiting • Poor weight gain • Colic • Fractious, fussy, crying • Irregular bowel actions
NEC What is it? • Infection of the mucosal lining of the bowel • Lactobacilli • Clostridium • Unknown
Who does it effect? • Maternal factors • prematurity • Hypoxic episodes • Cardiac anomaly • Exchange transfusion • Umbilical line near mesenteric artery • High osmolarity feeding • Increasing feeds quickly
Signs and symptoms • Change in behaviour • Subtle signs • Lethargy • Increasing naso-gastric aspirates • Labile temperature, labile blood sugars • Vomiting, bile later • Blood in stools • Abdominal distension
Later • Mottled, grey, capillary refill <4 secs • Apnoeic • Bradycardia • Oxygen requirement • Abdominal tenderness • Oedema • Dilated abdominal veins, dilated loops of bowel • Flare around umbilicus
Even later • Thrombocytopenia • Raised CRP • Pneumoperitoneum • Collapse, ventilation • Abdominal drain • Surgery, stoma’s • Short bowel
What to do • Large ng tube, aspirate and free drainage • Nil by mouth • IVI, Antibiotics • Blood sugar monitoring • Sepsis screen. Blood gas, FBC, U/E’s, Blood cultures • Urine MC/S, CXR, AXR
Types of oesophageal atresia and fistula 86% 7% 4%
Types continued 1% <1 <1
History • First case recorded Durston (1670) • Gibson (1697) first recorded with fistula • Ladd (1939) first staged repair • Height (1941) first successful primary repair.
Survival • Survival rate of around 90% • Incidence 1: 4500 • Antenatal diagnosis – polyhydramnios and absent stomach 56% predictive of OA.
After birth • Large NG tube • CXR, AXR • Replogle tube, 10 min suction to pharynx
Associated anomalies • 50% associated anomalies • Cardiac 29% • Vertebral, Anorectal, Cardiac, Tracheo, Oesophageal, Renal, Limb
Table 1 • Cardiovascular 29% • Gastro intestinal (anorectal 14%) 27% • Genito urinary 13% • Vertebral and skeletal 10% • Respiratory 6% • Genetic 4%
Primary repair • Paralyse and ventilate 5 days post op • Long gap – gastrostomy and assessment of gap, may leave 6 – 12 weeks before primary closure. • Gap of more than 6-8 vertebrae, oesophageal replacement
Post operation- early complications • Anastomotic leak , 27%, 24 – 72hrs • Anastomotic stricture • Recurrent tracheo oesophageal fistula
Late complications • Tracheomalacia • Gastro oesophageal reflux • Respiratory problems • Motility disorders • Growth
Definition • Rickham (1967) – an extensive resection to maximum of 75cm • Kuffer (1972) – 15cm with ileocaecal valve - 38cm without ileocaecal valve • Dorney (1985) – 11cm with I/C valve or 25cm without I/C valve
Introduction • Most common cause of intestinal failure. • NEC, Congenital atresia, Gastroschisis and volvulus. • Promote adaptive response through enteral feeding and careful management of TPN.
What is SBS • Reduced bowel surface area for absorption of nutrients together with rapid transit of intestinal contents. • TPN reduced as enteral feeds are introduced. • Need to promote intestinal adaptation.
Motility • The IC valve and colon is important to slow intestinal transit. • Proteins, Fats and Carbohydrates are absorbed almost completely within first 150cm of small bowel.
After resection. • Increase gastric emptying. • Ileal resection, increased transit time • An intact IC valve prolongs gut transit, loss of this causes an increase. • If colon resected transit increases.
How does the bowel adapt? • Cellular hyperplasia • Villous hypertrophy • Intestinal lengthening • Altered motility • Hormonal changes • Takes approx 2 years to reach max effect.
Central line complications • Infection • Thrombosis • Break in catheter • Air embolus • Tissue necrosis • Malposition • Cardiac tamponade
It takes approximately two years to achieve some normal diet
Gastroschisis • NEC • Bowel atresia, stenosis, web, duplication cyst • Meconium ileus • Jejunostomy, ileostomy, colostomy.
Bowel atresia, stenosis, web, duplication cyst • Interruption in the bowel • Effects motility • Adhesive bowel obstruction • Nil by mouth again
Meconium ileus • Thick, sticky meconium, secretions • Perforation or not (Ileum) • Stoma • Absorption, enzymes, EBM
Jejunostomy • High stoma • Trophic feeding, EBM, Donor EBM • Electrolytes • Six weeks reversal
Ileostomy • High or low • Milk • Stomal diarrhoea • Electrolytes • Prolapse, inversion, sore, thrush • Failure to thrive
Colostomy • Milk • Prolapse, inversion, soreness, • Diarrhoea • Constipation • Electrolytes
Important issues • Temperature • Fluid and electrolytes • Glucose • Management of reflux • Speech and language therapy • family
Management of gastro- oesophageal reflux • Thick n easy, Thix od • Gaviscon • Erythromycin • Domperidone • Ranitidine • Omeprazole