Download

1 / 18
180 likes | 262 Views
Toward a molecular intra-operative diagnosis of SLN invasion. R Garrel 1 , V Burcia 1 , J Solassol 2 , V Costes 3 , E Barbotte 4 , D DeVerbizier 5 , C Cartier 1 , M Makeieff 1 , L Crampette 1 , N Boulle 2 , T Maudelonde 5 B Guerrier 1 . Montpellier ’s Teaching Hospitals FRANCE

E N D
Toward a molecular intra-operative diagnosis of SLN invasion R Garrel1, V Burcia1, J Solassol2, V Costes3, E Barbotte4, D DeVerbizier5, C Cartier1, M Makeieff1, L Crampette1, N Boulle2, T Maudelonde5 B Guerrier1 . Montpellier’s Teaching Hospitals FRANCE 1 ENT, 2 Molecular Biology, 3 Pathology, 4 Biostatistics, 5 Nuclear Medicine
Sentinel Lymph Node technique : sampling method • Lymph node Mapping • Lymphoscintigraphy • Lymph node Biopsy • Lymph node Analysis • Serial sections + Immunohistochemistry
Goals of SLN technique • staging improvement: • Full histopathological analysis 2. select the right treatment for the right patient • to limit neck dissections to pN+ cases only : ≈ 30% patients
Limitation • The lack of accuracy of the Intraoperative diagnosis • “the Missing Link” • Sensitivity of routine Frozen section • 20 % sensitivity * • In best hands with serial sections : 90 %** • but • loss of materials • Not applicable in routine second surgery *Burcia et al. Otolaryngol Head and Neck Surgery 2010 **Tschopp et al. Otolaryngol Head and Neck Surgery 2005
The Role of molecular diagnosis ? • Advantages of molecular diagnosis for SLN staging Q-PCR • Not operator dependent • Automated → quicken → intraoperative use Questions are : #1 “Is the molecular staging as accurate as the gold standard ? ”. #2 “Which is the best Q-PCR marker ?”
....................................................Garrel et al. Clinical Cancer Research 2006............................................ Act 1 : Comparison between Q-PCR and Histopathology
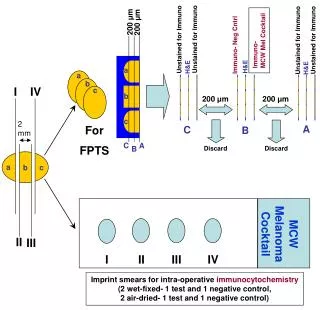
Matched analysis Snap frozen section Cyto imprint IHC • 3 cytokeratins : CK 5, 14 et 17 Q-PCR SN sections: 5µm/250µm
Q-PCR values / Size of SLN metastasis Garrel et al. Clinical Cancer Research 2006
Patient Staging (18 patients -71 SLN) = cutoff SN- SN+ Garrel et al. Clinical Cancer Research 2006
Key points • Results: • Q-PCR staging was as accurate as IHC: • positive neck vs negative neck: 100% se / sp • Background noise • No detection of minute micromestasis < 450 µm • in two patients but this inaccuracy was negated by the presence of larger metastases in another SLN being Q-PCR positive in the same two patients • Discriminatory power of Q-PCR is depending on the marker
Literature: Q-PCR markers • Screening of 40 potential markers using primary tumor and gross metastatic deposits compared with benign nodes • Ferris Cancer Res et al. 2005.
Second run of Q-PCR (23 patients-85 SLN) • Comparison of the three markers • Pemphigus Vulgaris Ag / SCCAg / CK 17 • Q-PCR with absolute quantification (plasmide)
Patients neck Q-PCR staging 1000000 100000 6 10000 1000 100 4 10 1 13 0 SLN – (n=17) SLN + (n=6) 1000000 100000 10000 6 1000 1 100 10 12 1 4 0 SLN – (n=17) SLN + (n=6) 1000000 100000 6 10000 3 1000 13 100 10 1 1 0 SLN – (n=17) SLN + (n=6) CK 17 Cutoff value 562 SCCA Cutoff value 48 PVA Solassol and Garrel BJC 2010 Cutoff value 562
ROC curvesanalysis CK17/ SCCA/ PVA →Pemphigus Vulgaris Ag +++ 100% area under curve 1.00 0.75 Sensitivity 0.50 0.25 PVA (AUC=100) SSC (AUC=97.9)) CK T17 (AUC=93.8) 0.00 0,00 0.25 0.50 0.75 1.00 1-Specificity Solassol and Garrel BJC 2010
Conclusion: PVA as the best Q-PCR marker • Larger cohorts to validate PVA for Q-PCR diagnosis • Evaluate the inter-laboratory variations of accuracy Micrometastasis Macrometastasis • “path the way toward the intraoperative molecular staging of sentinel lymph nodes in head and neck squamous cell carcinomas”
Future study assessment of automated technique • Q-PCR • one-step nucleic acid amplification (OSNA) OSNA CK19 → PVA SN in Head and Neck as the gold standard ?