Download
1 / 17
170 likes | 271 Views
PCT Fitness for Purpose – Creating Development Plans. PCT Fitness for Purpose – Development Plan. Development Plan Consultant’s Manual – September 2006. Manchester PCT – March 2007. 1. 1. Data management. 1. Financial review. Referral management. 2. Health review. 2.

E N D
PCT Fitness for Purpose – Creating Development Plans PCT Fitness for Purpose – Development Plan Development Plan Consultant’s Manual – September 2006 Manchester PCT – March 2007
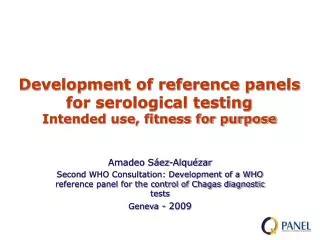
1. • 1. • Data management • 1. • Financial review • Referral management • 2. • Health review • 2. • Monitoring financial balance • 2. • 3. • Quality review • Optimise A&E/emergency care • 4. • Patient exp review • 3. • 5. • Progress review • Manage long-term conditions • 3. • Invoice review • 6. • Engagement • 7. • Integration of insights • 4. • Case management • 4. • Invoice adjudication • 8. • Pop. health goals • 5. • Intermediate care • 9. • Quality goals • 6. • Patient pathway redesign • 5. • Investigation • 10. • Patient exp goals • 11. • Financial goals • 7. • Improve access to diagnostics • 6. • Third party referral • 12. • CPM plan • 13. • Contracting • 7. • Effective payment • 14. • Monitoring plan • 15. • Completeness • 9. • Other initiatives • 8. • Activity volumes • 16. • Prioritisation • 10. • Practice-based commissioning • 17. • Outsourcing • 9. • Care and service levels • 18. • Financial plan • 10. • Patient satisfaction • 11. • Quality of outcomes • 12. • Clinical processes • 13. • Health status outcomes • Lower importance KEY Step 1a. - Question to the Executive Management Team: What are the most important capabilities to strengthen, if Manchester PCT is to be in the best position to improve the health & services as a commissioner? • Medium importance • High importance • Care pathway management • Monitoring • Provider management • Strategic planning • 1. Primary care • Build/analyse fact base • Define negotiation strategy • Execute negotiation process • Manage/develop provider market/capabilities • 2. Secondary care • Build/analyse fact base • Define negotiation strategy • Execute negotiation process • Manage/develop provider market/capabilities • 8. • Health improvement protection/equity • 3. Social care • Build/analyse fact base • Define negotiation strategy • Execute negotiation process • Manage/develop provider market/capabilities • 4. Tertiary care • Build/analyse fact base • Define negotiation strategy • Execute negotiation process • Manage/develop provider market/capabilities • 5. Mental Health • Build/analyse fact base • Define negotiation strategy • Execute negotiation process • Manage/develop provider market/capabilities Source: PCT Fitness for Purpose Diagnostic; PCT management team; team analysis
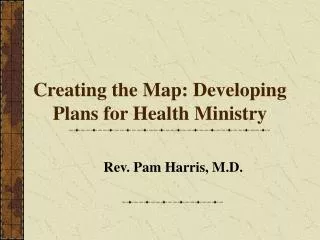
1. • 1. • Data management • 1. • Financial review • Referral management • 2. • Health review • 2. • Monitoring financial balance • 2. • 3. • Quality review • Optimise A&E/emergency care • 4. • Patient exp review • 3. • 5. • Progress review • Manage long-term conditions • 3. • Invoice review • 6. • Engagement • 7. • Integration of insights • 4. • Case management • 4. • Invoice adjudication • 8. • Pop. health goals • 5. • Intermediate care • 9. • Quality goals • 6. • Patient pathway redesign • 5. • Investigation • 10. • Patient exp goals • 11. • Financial goals • 7. • Improve access to diagnostics • 6. • Third party referral • 12. • CPM plan • 13. • Contracting • 7. • Effective payment • 14. • Monitoring plan • 15. • Completeness • 9. • Other initiatives • 8. • Activity volumes • 16. • Prioritisation • 10. • Practice-based commissioning • 17. • Outsourcing • 9. • Care and service levels • 18. • Financial plan • 10. • Patient satisfaction • 11. • Quality of outcomes • 12. • Clinical processes • 13. • Health status outcomes • PCT rating • Key Step 1b – How does the importance match up with Manchester PCT’s diagnostic scores? • Needs significant improvement • Meets minimum standards • Good to best practice • Care pathway management 1 2 3 1 2 3 1 2 3 1 2 3 • Monitoring • Provider management • Strategic planning • 1. Primary care • Build/analyse fact base • Define negotiation strategy • Execute negotiation process • Manage/develop provider market/capabilities • 2. Secondary care • Build/analyse fact base • Define negotiation strategy • Execute negotiation process • Manage/develop provider market/capabilities • 8. • Health improvement protection/equity • 3. Social care • Build/analyse fact base • Define negotiation strategy • Execute negotiation process • Manage/develop provider market/capabilities • 4. Tertiary care • Build/analyse fact base • Define negotiation strategy • Execute negotiation process • Manage/develop provider market/capabilities • 5. Mental Health • Build/analyse fact base • Define negotiation strategy • Execute negotiation process • Manage/develop provider market/capabilities Source: PCT Fitness for Purpose Diagnostic; PCT management team; team analysis
Rationale for Prioritisation – 1/2How were priority areas agreed? • In order to make progress the Executive Management Team (EMT) were clear that the • number of priorities should be realistic (around 10): spreading effort amongst too many • priorities could dilute the impact Manchester PCT requires. • In prioritising where to begin work first the EMT looked at the FfP diagnostic areas without the • scores and considered which areas were of high and medium importance in terms of what • would make the biggest impact for Manchester PCT. They were conscious that • in some areas that had low scores within the assessment phase, a great deal of progress • could now be evidenced. • The next stage was to look at the scores & the evidence of recent progress and ask: • Where do we have low scores and high importance? (Answering this question identified the high priority capabilities to work on immediately) • Where do we have low scores and medium importance? (Answering this question identified the medium priority capabilities to work on ‘down the road’) • Where do we have good scores & either high or medium importance? (Answering this question identified possible areas where the PCT would like to strengthen from ‘good’ to ‘great’)
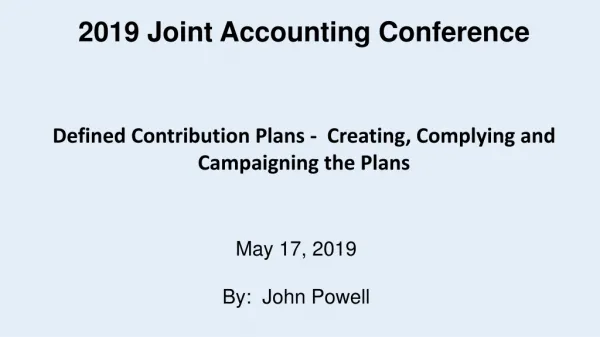
Prioritisation matrix: Key: Priority Numbers • Immediately needed • Address in timely way • Prioritisation matrix 1.2 • Define negotiation strategy PC 1.1 X*.1 6 • Build/analyse fact base PC • Large 1.4 1 • Manage/develop provider market/capabilities PC 13 2.1 1.2 1.4 2.3 10 4 • Build/analyse fact base SC 2 11 2.3 • Execute negotiation process SC 3.1 • Build/analyse fact base Soc. Care 3 18 4.1 • Build/analyse fact base TC 1 8 • Data management 6 1 5.1 8 • Build/analyse fact base Mental Health • Activity volumes 1 4 • Invoice adjucation 1 • Referral management • Size of gap 10 10 2 • Patient satisfaction • Optimise A&E / Emergency care 13 2 6 • Patient pathway redesign 3 • Quality review 1 • Financial review 6 • Engagement 18 11 • Financial plan • Financial goals 13 • Small • Contracting • Maintain current performance • Lower • Medium • High 13 • Move to best practice, if possible • Health status outcomes • Relative importance to PCT commissioning purpose 2 • Monitoring financial balance Key to circle colours: 10 • Practice-based commissioning • Circled items where there are related areas • FfP Diagnostic Category: Strategic planning • FfP DiagnosticCategory:Care Pathway Management • FfP DiagnosticCategory:Provider Management • FfP Diagnostic Category: Monitoring *1.1, 2.1, 3.1, 4.1, 5.1
Strategic planning • Care Pathway Management • Provider Management • Monitoring The 11 prioritised diagnostic elements are addressed through 8 specific and 4 cross-cutting themes • Big solutions • FfP Diagnostic Element • Key Themes • Contracting 1.2 • Primary care – define negotiation strategy • Secondary care – execute negotiation strategy 2.3 • Contracting 13 1 • Data management • Data management 8 • Activity volume 1.4 • Developing capability of existing and new providers • Primary care – manage/develop provider market/ capabilities • Care Pathway Management 1 6 • Referral management/Patient pathway redesign 2 • Optimise A&E/emergency care • Emergency care 3 • Clinical quality review • Clinical quality review • Engagement • Engagement – PPI 6 11 • Financial goals • Modelling + Data mgmt • Cross-cutting themes • Strategic route map • Performance management • Becoming a confident commissioner • Business processes
Rationale for Prioritisation – 2/2Some ‘low score’ areas are not addressed as either ‘red’ or ‘amber’, why? • Strategic Planning • Patient Experience Review & Patient Experience Goals required the ‘Engagement’ work 1st • Progress Review has been initiated with the establishment of the Performance Directorate • and a review of the existing performance management systems • Integration of insights internally was judged not as important as integrating insights between PBC and • the PCT Directorates and would be tackled from this perspective • As ‘Quality Review’ was a high priority together with the recent progress evidenced at the • Board on clinical quality systems, Quality Goals would not be addressed separately • Monitoring Plan, Completeness, Prioritisation & Outsourcing would be returned to at the 12 • month review. It was judged that both the work from other high priority areas & the adoption • of ‘best practice’ from the previous, three PCTs would impact positively on all four areas • Care Pathway Management • Improve access to diagnostics capability had been recently reviewed. Greater focus was now • in place & evidenced progress had been made since the assessment phase • Provider Management • Much of this section would follow on from progress made on the areas prioritised ‘red’/’amber’ • Monitoring • Investigation processes would be reviewed when progressing ‘Invoice Adjudication’ (‘amber’) • The areas of Patient Satisfaction, Quality of Outcomes & Clinical Processes formed part of • the comprehensive Quality Review plan (linked to the mitigation plan for Clinical Quality, • previously requested by the SHA)
OVERVIEW: A development plan for Manchester PCT that is driven by a clear vision and built on strong organisational foundations • DEVELOPMENT ACTIONS: DEVELOPMENT THEMES: • VISION Synthesise and communicate • STRATEGIC ROUTE MAP • STRATEGIC LEVERS Align and communicate • PCT’s role in market development • Quality • Use of CHOICE • Risk transfer • Role of PPI • STRATEGY Define strategy for • Engagement • Commissioning (Emergency care, Referral management) • Contracting/negotiation • Clinical quality • Developing providers • Disease areas • Sectors • Initiatives • Data Management • Performance Management • Becoming a confident commissioner • Business processes • Modelling for business support Build and disseminate good practice • ORGANISATIONAL STRENGTHS
Summary of the Manchester PCT Development Plan 1/3 • Big solutions: products, impacts & lead Director • Metrics • Publication of PCT Prospectus in line with National guidance (July 2007) • Inclusion of strategic priorities within business plans & personal objectives (07/08) • Strategic Route Map – LAURA ROBERTS • Capture vision and strategy in concise, 2 • Identified set of strategic levers • Clear description of how levers work together • Incentives & expectations in line with strategic objectives & business goals (audit of Directorate & Individual objectives) • Improved PCT performance as judged by the SHA • Performance Management – IAIN BELL • Greater focus at all levels of PCT on outputs & outcomes – a business feedback system • Individual responsibilities clearly defined/publicised/actioned • Business Processes – ZOE COHEN • Matrix working for key business priorities – staff know how to do this • Manchester PCT Project Management methodology being used • Business case format and process established • Increase in the % of projects delivered to time • Reduced number of projects cancelled or delayed due to poor initial evaluation &/or lack of realistic prioritisation • Improvement on baseline perceptions of key partner organisations • Improvement on relevant questions within the National Staff Survey (from 2006/07) • Becoming a Confident Commissioner – ZOE COHEN • Increased credibility perceived by staff & key partners (PCT Staff, MCC, Hospitals, GPs) of the PCT’s ability to commission • Accuracy of capacity planning model to • within +/- 5% tolerance for all forecasts. • Increase in the proportional spend on • Primary, Community & Preventative Services • Modelling for Business Support – GARY RAPHAEL • Identified ‘health impact’ modelling resource • Greater agreement & action from providers on change
Big solutions: products, impacts & lead Director • Metrics • Data Management – IAIN BELL • Health intelligence service • Well used set of information products • Better informed ad hoc requests • Intelligence team proactively generating new business insights • Financial Goals & Contracting – GARY RAPHAEL • Explicit VfM strategy, improved negotiation on VfM, proactive monitoring of contracts, greater use of plurality of providers • Primary Care Performance Tables • Clinical Quality Review – RAJAN MADHOK • Quality Assurance system for all contracts • More robust approach to patient safety • Tighter approach to poorly performing clinicians • Engagement (with Patients & the Public) – ZOE COHEN • Targeted PPI impact aligned to strategy • Patient Experience Metrics • Integrated PALs & Complaints Service • Patient experience outcome indicators in place for contracts by 2008/09 • Increased involvement of patients & the Public within service redesign work Summary of the Manchester PCT Development Plan 2/3 • Increase in accuracy of data within monthly • reports • Decrease in the number of multiple requests • Regular generation of new commissioning • improvement hypotheses • Realise aminimum of 1% of PCT income • (annually) from improved efficiency/ productivity • (in line with National benchmarks) • Qtr on Qtr increase on £s saved & reinvested • from contracts • Clinical outcome indicators in 08/09 contracts • Increased reporting of clinical incidents ( next • 12 months) • Improved response time to incident reporting
Big solutions: products, impacts & lead Director • Metrics • Care Pathway Management - SARA RADCLIFFE • Standard KPIs on key care pathways available to PBC • Demand as a consequence of appropriate interventions • Optimising A&E/Emergency Care – SARA RADCLIFFE • New contract for short stay Emergency Medical Admissions (EMAs) • AED triage owned by Primary Care • Improved delivery of alternatives to EMAs • Develop Capability of Existing/ New Providers – SARA RADCLIFFE • Clear corporate view on the role of competition as a strategic lever • An accreditation process for new providers • Identified stronger providers gaining more of the business (particularly in Primary Care) Summary of the Manchester PCT Development Plan 3/3 • Increase in the number of conditions dealt with outside of an acute hospital, within primary care • Quicker access to initial diagnostics and treatment in and outside of hospital (as part of • 18 week target monitoring) • Reduced growth in acute admissions and A&E attendances • Reduction in the ‘actual’ to ‘expected’ ratio of emergency admissions for Ambulatory Care Sensitive Conditions • Market development intentions published • Increase in the number of providers able to deliver extended care (to accreditation spec) outside of an acute hospital (on 2006/07 baseline)
Manchester FfP Development Plan – Summary (1/4) • 2007 • 2008 • Action owner • 3 • 4 • 5 • 6 • 7 • 8 • 9 • 10 • 11 • 12 • 1 • 2 • 3 • 4 • 5 • 6 • 7 • 8 • 9 • Activity Laura Roberts • Strategic route map 2 page PCT strategic vision • Synthesize vision Clear explanation of how PCT use levers • Develop strategic levers • Performance management Intentions published • Each directorate, creates mandate based on PCT’s strategic objectives Iain Bell All Directorates trained, baselines recorded • Establish a performance management function • Make performance management (PMg) part of new employee induction Established in Induction All JDs include PMg • Include performance management activities in managers’ job description End of 1st round of training–all action leads • Train staff on use of performance accelerator (PA) PA fully populated • Set up and populate performance accelerator with goals PA review aligned with annual objective setting • Design process to monitor against goals (KPIs) • Business processes Zoe Cohen • Establish formal business processes for key areas 1st Priorities identified • Identify and sign off priority areas 1st Priorities mapped • Map current processes Improvements identified, action allocated • Identify and implement improvement measures Skill gaps identified • Support efficient cross-directorate work streams • Improve project management (PM) skill level 1st draft of PM system • Develop standardised preparation and kick off processes PM system in use • Set up performance management for project skills
Manchester FfP Development Plan - Summary (2/4) • 2007 • 2008 • Action owner • 3 • 4 • 5 • 6 • 7 • 8 • 9 • 10 • 11 • 12 • 1 • 2 • 3 • 4 • 5 • 6 • 7 • 8 • 9 • Activity • Data management Detailed programme plans Iain Bell • Create mandate Team in place • Set up ‘business as usual’ team First set of dashboards • Create management dashboards Work programme published • Establish Business Intelligence (BI) programme System trialled • Set up system to automate and improve BI programme Synthesis team in place • Set up ‘synthesis team’ Processes set up plus feedback mechanism for users • Establish and market analytical service to handle ‘ad hoc’ requests • Becoming a confident commissioner Zoe Cohen Baseline perceptions completed • Assess communication needs Initial set drafted • Create key messages re. PCT vision & strategy • Train staff on use of messages Account holders identified • Identify/create customised channels Team set up • Modelling Gary Raphael • Set up multi-disciplinary modelling team • Determine which capacity is required 2nd iteration 1st iteration • Create models to simulate impact of redesign on patients and resources-AED/EMA priority Plan published • Develop modelling support for priority business processes
Manchester FfP Development Plan - Summary (3/4) • 2007 • 2008 • Action owner • 3 • 4 • 5 • 6 • 7 • 8 • 9 • 10 • 11 • 12 • 1 • 2 • 3 • 4 • 5 • 6 • 7 • 8 • 9 • Activity Best practice system implemented • Clinical Quality Review Rajan Madhok • Governance processes (structure and format) • Specifications • Metrics • CQ metrics in • Contracts • System • Quality assurance systems (all contracts) Metrics Implemented • Patient safety system System reviewed Implemented • Poorly performing clinicians process Sara Radcliffe Project Management Leadership Teams set up Agree with PBC • Care Pathway Management • Create framework for care pathway development Published • Identify high impact pathways Draft pathways • Formulate care pathways Prototype system • Feedback system for PBC New Triage model agreed Sara Radcliffe • Optimising AE/Emergency Care Top level alternative flow model • Restructure partnership with SC Local Plans 1st phase implemented • Create common framework & local hub plans • Improve supply/demand for urgent care Decision on IC expansion New IC criteria Zoe Cohen • Engagement Policy approved • Mainstream PPI Toolkit launched Database in place • Dedicate enabling capacity Engagement mechanisms agreed • Develop effective community engagement Single function • Create merged PALs/complaints
DRAFT – Manchester FfP Development Plan (4/4) • 2007 • 2008 • Action owner • 3 • 4 • 5 • 6 • 7 • 8 • 9 • 10 • 11 • 12 • 1 • 2 • 3 • 4 • 5 • 6 • 7 • 8 • 9 • Activity Draft Criteria Clear strategic role • Developing capability of existing and new providers Draft process Sara Radcliffe • Set up accreditation mechanism Plan published • Adopt balanced approach to creating stronger capabilities • Expand poor performance review process • Create a cross-Directorate function for providers who have queries/need support to provide new services Review existing process Launch new process Support Service available Identified strategic ’team’ • VfM as part of the strategy Gary Raphael Strategic VfM plan 08/09 onwards • Establish collaboration across directorates • Identify VfM areas for year ahead Team in place • Improve negotiation for VfM: Secondary Care (SC) Gary Raphael • Team for negotiation Clearer contracting process • Contracting process SC comprehensive profiles • Build provider profiles Key flex/freeze efficiencies identified • Tighten contracts 1st success stories • Engage GPs PBC sponsored strategic VfM team Gary Raphael • Develop a clear vision for a Primary Care (PC) negotiation strategy PC Strategy • Obtain vision re. strategic route map & translate for PC Principles published • Establish negotiation principles Function established • Create a single function for negotiating PC 2nd cycle of reporting • Primary Care KPIs developed • KPI reporting Made available to the public • Publishing valid KPIs
FfP Development Plan - Governance structure SHA NEDs/PCT board • Bi-monthly exception reporting to the Board • 6 monthly full review of progress to • Governance Committee CE Laura • Accountable to SHA and PCT board • Strategic route map • Part of usual business; fortnightly exceptions via • EMT business meetings Project Mgr Leads Finance Gary Corp. Affairs Zoë Commission Sara PH Sally Med. Dir.Rajan OperationsJohn PerformanceIain Manages project plan • Monitors/supports implementation • Prepares reports • Accountable to CE • Ensure timely completion of tactical action within diagnostic element • Modelling • Financial Goals & Contracting • Business processes • Becoming a confident commissioner • Engagement /PPI • Care Pathway management • AE/ Emergency care • Developing capabilities of new and existing providers • Clinical quality review • Data management • Performance management