Download
1 / 36
370 likes | 699 Views
The Pharmaceutical Industry. Professor Vivian Ho Health Economics Fall 2009. Outline. Competitiveness of the pharmaceutical industry Conduct Performance. Benefits of Drugs. Reduce mortality Reduce morbidity/improve quality of life Reduce cost of treating diseases. Industry Structure.

E N D
The Pharmaceutical Industry Professor Vivian Ho Health Economics Fall 2009
Outline • Competitiveness of the pharmaceutical industry • Conduct • Performance
Benefits of Drugs • Reduce mortality • Reduce morbidity/improve quality of life • Reduce cost of treating diseases
Industry Structure • # and size distribution of sellers • Buyers’ side characteristics • Barriers to entry • Government regulation
Top 10 U.S. Prescription Drug Sellers, 2008 Company Sales $b Pfizer 20.5 GlaxoSmithKline 18.4 AstraZeneca 16.3 Johnson & Johnson 16.0 Merck & Co 15.5 Amgen 13.4 Hoffman-LaRoche (incl Genentech) 13.1 Novartis 12.4 Lilly 11.4 Sanofi-Aventis 11.0 http://www.imshealth.com
Can competition be accurate measured at the industry level? • Most drugs are not substitutes to the patient • The relevant product market is the therapeutic market • Only a few major drugs compete in most therapeutic markets • Concentration ratios at this level are higher than for industry as a whole
*Includes “Generics” as a top-4 firm Express Scripts Drug Trend Report, 2006
Buyers of Prescription Drugs, 2007 Expend. Source ($billions) Percent Total 227.4 100.0% All private 146.6 64.5 Out-of-pocket 47.5 20.9 Private insurance 99.1 43.6 All government 80.8 35.5 Federal 66.5 29.2 State 14.3 6.3 The Buyer Side
How 3rd parties influence drug demand • Even if consumers exert little influence over drug choice, 3rd parties are making the market more competitive • Formularies - list of selected drugs physicians may prescribe • Used by hospitals to limit inventories and costs • Used by most HMOs and many PPOs • Used by many state Medicaid programs
Drug utilization review • Used by insurers to enforce formularies, identify inappropriate prescribing practices • Government influence • 1990 Omnibus Budget Reconciliation Act - Federal funding provided for drug only if state Medicaid program receives manufacturer rebate agreement
Government influence (cont.) • 1992 Veterans Health Care Act - price discounts for Federal Supply Schedule, VA, Dept. of Defense • These programs may restrict costs for government, but drug firms may be forced to raise nonfederal prices
“…managed care emphasizes less-expensive, preventive types of treatment” “The rate of growth for drugs to treat high blood pressure and high cholesterol in certain managed-care strongholds on the West Cost has gone off the charts” WSJ 10/17/96
“Consumers in the $94 billion prescription drug market are mostly indifferent to price. What will happen when they all become budget conscious? Forbes 4/5/99
Pharmacy Benefit ManagersGeneral Strengths • Intermediaries that purchase drugs from manufacturers and pharmacies at a reduced price for health insurers • PBMs provide drugs at lower costs • Achieve econ. of scale in pharmacy benefits by serving multiple plan sponsors • Large market share on buyer’s side stronger negotiating power w/ drug companies
Pharmacy Benefit ManagersGeneral Strengths • PBMs can use their patient information to their strategic advantage • e.g. Medco’s 60m patients • How drugs prescribed, used, impact on disease • Can prevent inappropriate drug interactions, under/over medication
Vertical Integration • Brand name drug companies were purchasing PBMs
Vertical Integration • Good or bad idea? • Buy the information, not the PBM • “Industry consultants and Medco competitors argue that Merck could have bought that information from Medco or others in the field without buying the company.” NYT 8/5/93 • Critics argue that PBMs will only serve to lower prescription pharmaceutical prices
Vertical Integration • Comments from Roy Vagelos, former Merck CEO • “In classic terms of competition, we could see that the power of the buyers was growing…PBMs were…bringing together the person who chooses the drug and the person who pays for the drug.” • “Having salespeople visit doctors’ offices does not allow us to reach PBMs, HMOs, or plan sponsors -- the major players in the emerging market.”
Vertical Integration • Merck bought Medco as a response to managed care • Strategic attempt to market power. How? • Followup on patients w/ chronic illness who may stop taking prescribed meds • Position Merck drugs favorably on formulary • e.g. lower patient copay, or lower cost to plan sponsor
Vertical Integration • In 2001, Medco accounted for $26b of Merck’s $46b sales • Medco filled 537m prescriptions in 2001 • But profit margins for Medco <3%
Vertical Integration • Regulators worried that patients and employers would be hurt by this type of vertical integration • Regulators required separate management of drug sales and PBM operations • Merck spun off Medco in 2003
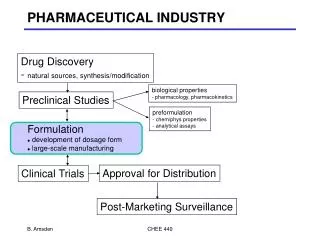
Role of the FDA • The Food and Drug Administration approves a new drug before it can be sold in the marketplace • Also determines whether drugs require a physician prescription vs. OTC sales • The FDA requires extensive, costly testing before approving a drug • What is the economic argument for the FDA’s role?
Role of the FDA • Type 1 error: The FDA rejects the application for a new drug that is truly safe and effective • Type 2 error: The FDA approves a drug that is unsafe or ineffective • If you worked for the FDA, which error would you rather make? • Why?
Role of the FDA • On Sept 20 2004, Merck announced it was recalling Vioxx, its $2.5b-a-year arthritis medicine • Was shown to double the risk of heart attacks and strokes in long-term users • Merck lost 27% of its total market capitalization in the stock market ($27b) in one day
Role of the FDA • Can we compare the benefits of allowing novel, risky drugs on the market to the costs? (Olson, 2004) • “Novel” drugs offer therapeutic gains over existing remedies • 1st of a kind in a therapeutic area (e.g. Viagra) • New additions to an existing class, which are safer or more effective (e.g. Celebrex)
Role of the FDA • Adverse drug reactions (ADRs) • Severe reactions to drugs that are fatal, life-threatening, permanently disabling or require hospitalization • Most ADRs filed by physicians and other health professionals, reported to drug’s manufacturer or the FDA • Data is collected in the FDA’s spontaneous reports system
Role of the FDA • The stock of novel drugs introduced 1990-1995 was estimated to result in 1.7m life years saved • (Predicted deaths avoided per drug) x (estimated life years gained per drug) x (# novel drugs) • 137,000 life years lost due to ADR deaths during this time period • (Predicted deaths due to ADR per drug) x (life years lost per drug) x (# novel drugs)
Role of the FDA • Losses due to ADRs may be underestimated • Only ADR deaths in 1st 2 years after FDA approval were considered • ADRs may be underreported • Many ADRs do not cause death, but result in hospitalization or serious disability • Is the FDA being too lax or too lenient in approving new drugs?
Barriers to entry • Government patents • Brand loyalty advantage • Control over a key input
Government Patents • Innovating firm gains the right to be sole producer of a drug for legal maximum of 20 years • Preserves incentives for firms to undertake risky and costly research and development (R&D) that is socially valuable • Rationale: Monopoly restriction of output better than having no output at all
Monopoly power of patents is not always strong • Patents granted for chemical composition, not therapeutic novelty • Lipitor, Crestor, and Zocor all compete in the cholesterol-lowering drug market • Significant part of patent life may be spent trying to get FDA approval • “effective” patent life = 8 years
Monopoly power of patents is not always strong • 1984 Waxman-Hatch Act - benefits for both brand-name and generic companies • Effective life of new drug patent can be extended up to 5 years if FDA delayed market introduction • Fast approval process for generics: eliminated proof of safety & effectiveness