Download
1 / 31
310 likes | 315 Views
Our mission is to create a healthcare model that integrates primary with secondary and tertiary healthcare, making it accessible and affordable to both urban and rural areas in North-East India.

E N D
MISSION STATEMENT : TO CREATE A HEALTHCARE MODEL WHICH WILL INTEGRATE PRIMARY WITH SECONDARY & TERTIARY HEALTHCARE & MAKE IT ACCESSIBLE & AFFORDABLE TO URBAN AS WELL AS RURAL NORTH-EAST
WHAT PROMPTED US TO THINK OF A MODEL LIKE THIS ? INSPITE OF A SPURT IN THE NUMBER OF HEALTHCARE SETUPS IN THE PRIVATE / CORPORATE SECTOR IN THE NORTH EAST IN THE LAST DECADE, WE STILL HAVE OBSERVED THAT : • MOST PEOPLE WHO CAN AFFORD STILL GO OUTSIDE THIS REGION FOR SPECIALITY HEALTHCARE NEEDS – HUGE OUTFLOW OF RESOURCES, MANY PEOPLE WHO DO NOT HAVE THE RESOURCES BORROW / SELL OFF THEIR ASSETS TO GO OUT OF THE REGION FOR SPECIALTY HEALTHCARE • PEOPLE WHO CANNOT AFFORD HAVE NO OPTION
QUALITY & EFFECTIVE HEALTHCARE FACILITIES ARE YET TO PENETRATE MANY AREAS • MEDICAL TREATMENT IS STILL VERY EXPENSIVE IN THIS REGION • FOCUS ON ACADEMIC RESEARCH IS VERY LESS : VERY FEW RESEARCH PUBLICATIONS IN NATIONAL / INTERNATIONAL MEDICAL JOURNALS /PERIODICALS • IT IS A MATTER OF SERIOUS DEBATE AS TO WHETHER WE HAVE BEEN ABLE TO ACHIEVE STANDARDS COMPARABLE TO INSTITUTIONS IN MANY OTHER PARTS OF THE COUNTRY
A CUMULATIVE EFFECT RESULTING IN : • NO SIGNIFICANT IMPROVEMENT IN SPECIALITY SECONDARY & TERTIARY HEALTHCARE • INABILITY TO ATTRACT / RETAIN QUALITY MANPOWER • A HUGE SCOPE FOR LOTS OF IMPROVEMENT IN MANY SPECIALITY / SUPER-SPECIALITY AREAS LIKE : • INFECTIOUS DISEASES IN CHILDREN • PAEDIATRIC INTENSIVE CARE • DEDICATED BURNS MANAGEMENT • PLASTIC & RECONSTRUCTIVE SURGERY • ONCOLOGY & ONCOSURGERY • HAEMATO-ONCOLOGY • CARDIO-THORACIC & VASCULAR SURGERY • INTERVENTIONAL CARDIOLOGY • INTERVENTIONAL RADIOLOGY • TRANSFUSION MEDICINE • GERIATRIC CARE • ORGAN TRANSPLANTATION, ETC
OUR MODEL A HEALTHCARE MODEL TO BE RUN BY A “TRUST/FOUNDATION”OFFERING HEALTHCARE FACILITIES WITH CROSS-SUBSIDIZATIONWITH A 3-TIER APPROACH :: • PAID FACILITIES • SUBSIDIZED FACILITIES • FREE FACILITIES A HEALTHCARE MODEL WHICH HAS BEEN VERY SUCCESSFULLY ADOPTED BY INSTITUTES LIKE LV PRASAD EYE INSTITUTE, HYDERABAD; ARAVIND EYE INSTITUTE, MADURAI ; SRI CHITRA TIRUNAL INSTITUTE OF MEDICAL SCIENCES & TECHNOLOGY, TRIVANDRUM ; NARAYANA HRUDAYALAYA, BANGALORE; ETC.
OUR MODEL WILL HOWEVER HAVE A FEW MORE UNIQUE & ADDITIONAL FEATURES OUR PROPOSED STRUCTURE : • A 500- 600 BED CENTRAL INSTITUTE BASED IN / AROUND GUWAHATI TO BE SET UP IN 3-4 PHASES WITH AN ATTACHED NURSING/PARA-MEDICAL TRAINING INSTITUTE • RURAL MOBILE OUTREACH MODULES • RURAL SMALL HOSPITALS& TELEMEDICINE MODULES CONNECTED TO THE CENTRAL INSTITUTE
A FEW UNIQUE FEATURES OF THE CENTRAL INSTITUTE STRUCTURAL DESIGNING AS PER “GREEN BUILDING STANDARDS” CONFORMING TO LEED RATING CRITERIA – WILL BE THE 1ST OF ITS KIND IN SPECIALITY HEALTHCARE SECTOR IN INDIA ADVANTAGES : • OPERATIONAL SAVINGS :40-50% LESS ENERGY CONSUMPTION, 20-30% LESS WATER CONSUMPTION, 15-20% REDUCED CLEANING & MAINTENANCE COSTS • ACCESS TO DAYLIGHT & VIEWS :IMPROVES PRODUCTIVITY BY 12-15% • AIR QUALITY :ALWAYS FRESH & HEALTHY
ALL OPERATION THEATRES WILL MODULAR STAINLESS STEEL CONFORMING TO WHO / NABH STANDARDS – 1ST OF ITS KIND IN ENTIRE NE REGION Features : • 100% STERILE AIR-PURIFICATION SYSTEMS • NO DUCT / MICROBIAL POCKETS INSIDE THE OTs • ALLOWS REMOVAL OF CONTAMINATED /INFECTED AIR WITHIN 2 SECS • BUILT-IN DEFUMIGATION SYSTEMS
Pneumatic System for Specimen & Drug Transport – 1st in Eastern India Advantages & Unique Features • Eliminates manpower & lift usage in transport of specimens from wards to laboratories , drugs from pharmacy, etc • This system connects the labs and the pharmacy to locations all over the hospital • Transporting blood from the blood bank to the blood bank satellite and operating room suite. • Saves a huge amount of time – completely computerised control system
Some More features :: • ENTIRE HOSPITAL WILL BE BUILT ON A MODULAR DESIGN– NEW MODULES CAN BE ADDED ANY TIME WITHOUT DISTURBANCE IN THE FUNCTIONING OF EXISTING MODULES • ENTIRE HOSPITAL WILL HAVECENTRAL GAS PIPELINE SYSTEM : NO TRANSPORT OF MEDICAL GAS CYLINDERS INSIDE THE HOSPITAL • INTEGRATED IT BACKBONE WITH 1000 MBPS LAN SPEED TO MINIMISE STATIONERY USAGE • LED LIGHTING SYSTEM FOR EFFICIENT ENERGY SAVINGS • FILMLESS HOSPITAL : CONNECTED THROUGH PACS(HUGE COST SAVINGS IN MEDICAL FILMS) • USE OF GENERIC DRUGS :SAVES A LOT OF NON-PRODUCTIVE EXPENDITURE
DEPARTMENTS IN THE CENTRAL INSTITUTE • GENERAL MEDICINE INCLUDING SUB-SPECIALITIES LIKE RHEUMATOLOGY, RESPIRATORY DISEASE, ETC • GENERAL SURGERY INCLUDING SUB-SPECIALITIES LIKE COLO-RECTAL SURGERY, LAPAROSCOPIC SURGERY, GI SURGERY, ETC • CARDIOLOGY WITH CATH-LAB FOR INTERVENTIONAL CARDIOLOGY • CARDIO-THORACIC & VASCULAR SURGERY • OBSTETRICS & GYNAECOLOGY • INFERTILITY CENTER • ENDOCRINOLOGY • GASTROENTEROLOGY • PAEDIATRICS • PAEDIATRIC SURGERY • INFECTIOUS DISEASES CENTER : 1ST IN NE • ORTHOPAEDICS & ARTHROSCOPY CENTER • NEUROLOGY
NEPHROLOGY • DIALYSIS CENTER • UROLOGY WITH LITHOTRIPSY CENTER • ONCOLOGY • ONCOSURGERY • PLASTIC & RECONSTRUCTIVE SURGERY • BURNS UNIT WITH BURN ICU : 1ST IN EASTERN INDIA • TRAUMA CENTER • DERMATOLOGY • ENT • OPHTHALMOLOGY
GENERAL ICU • CARDIAC ICU • NEONATAL ICU • PAEDIATRIC ICU • GERIATRIC CENTRE : 1ST IN NE REGION • MAXILLOFACIAL & ADVANCED DENTISTRY CENTER • TRANSFUSION MEDICINE WITH COMPONENT LEVEL BLOOD BANK • INTERVENTIONAL RADIOLOGY CENTER : 1ST IN NE • ANAESTHESIOLOGY & CRITICAL CARE • REHABILITATION CENTER
DIAGNOSTIC FACILITIES • RADIOLOGY & IMAGING :COMPUTED RADIOGRAPHY, IITV, ULTRASONOGRAPHY, COLOUR DOPPLER, CT WITH FLUOROSCOPY, MRI, NUCLEAR MEDICINE, DSA, BONE DENSITOMETRY, OPG, CEPHALOMETRY, DIGITAL MAMMOGRAPHY, ETC. • LABORATORY SERVICES :CLINICAL PATHOLOGY, HISTOPATHOLOGY, MICROBIOLOGY, BIOCHEMISTRY, HAEMATOLOGY, BLOOD GAS ANALYZER, ETC
ENDOSCOPY SERVICES :VIDEO ENDOSCOPY, ERCP, INTERVENTIONAL PROCEDURES • CARDIOLOGY :ECG, ECHOCARDIOGRAPHY, STRESS ECHOCARDIOGRAPHY, TMT, HOLTER, ETC • NEUROLOGY :EMG, NCV, SLEEP DISORDER CLINIC, ETC • ALL ALLIED DIAGNOSTIC SERVICESCONNECTED WITH OTHER DEPARTMENTS
High Tech Cardiac & Trauma Ambulances • This is a high end version of a trauma care centre. • This trauma unit is designed for deployment in situations requiring onsite care • It is essentially a compact mobile trauma unit for routine treatment of common field medical requirements & emergencies. • It has a comprehensive range of life support systems to save organs and maintain organ functions
LEADING NATIONAL / INTERNATIONAL MEDICAL SPECIALISTS IN THE MEDICAL BOARD • COLLABORATIVE TIE-UPSWITH LEADING NATIONAL & INTERNATIONAL MEDICAL RESEARCH INSTITUTES FOR CONTINUOUS MANPOWER & TECHNOLOGY UPGRADATION AS WELL AS ORGANISATIONS IN NON-PROFIT SECTORLIKE SMILE FOUNDATION, INTERPLAST, ETC FOR PARTNERING IN VARIOUS PROJECTS • A SEPARATE DEPARTMENT FORBIO-MEDICAL / BIOTECHNOLOGY RESEARCH / STEM CELL RESEARCH, ETC. IN COLLABORATION WITH A LEADING INSTITUTE LIKE IITG / IIT-KGP, AIMS COCHIN, SCTIMST TRIVANDRUM • INDUSTRY COLLARORATION FOR MEDICAL RESEARCH, CLINICAL TRIALS, BETA TESTING OF NEW TECHNOLOGY
PROJECT CONCEPTION , DESIGNING & IMPLEMENTATION This project has been conceived and designed by a “ Group of Doctors” from Assam who are from different medical specialties & have come back home after spending a considerable part of their professional careers in various reputed hospitals around India and will be joined once ready for implementation by many more doctors from this region who are studying / working in various reputed hospitals in different parts of India
Manpower for the Project In Our Model : • The Central Institute will be manned by a team of committed doctors who have worked /are working in various reputed hospitals around the country & having significant experience in their respective fields • We will also attract manpower from various reputed institutions around the country on a periodic basis • The doctors will be given a full role & involvement in designing, planning, execution, etc of the respective modules of the project • Full facilities for academic research • Develop a pool of trained manpower within a span of 1-2 years who can be deployed in the peripheral setups One of the biggest constraints in the NE region is a lack of manpower in Specialty & Super-Specialty areas
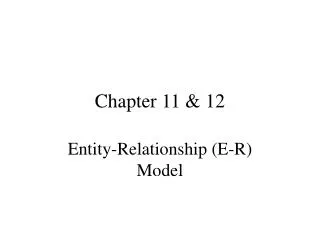
OUTREACH MODULES – PHASE I • 3 CLINICS IN THE 1ST PHASE WITHIN A RADIUS OF 100-150 KMS FROM THE CENTRAL INSTITUTE • OPD , ROUTINE DIAGNOSTIC FACILITIES , EDUCATION ON PREVENTIVE HEALTHCARE, ETC. IN INITIAL PHASE ATLEAST 2 DAYS / WEEK • CLINICS WILL BE MANNED BY DOCTORS FROM THE CENTRAL INSTITUTE • SCREENING & COUNSELLING OF PATIENTS REQUIRING SECONDARY / TERTIARY CARE
INFRASTRUCTURE OF THE OUTREACH MODULES IN THE INITIAL PHASE WILL BE COVERED BY FULLY EQUIPPEDMOBILE CENTRES HAVING FACILITIES LIKE : • BASIC OPD / SCREENING FACILITIES • MOBILE CR (DIGITAL X-RAY) • ULTRASONOGRAPHY & COLOUR DOPPLER • ECG • BLOOD COLLECTION FACILITIES • MINOR OPERATION THEATRE • PHARMACY • SCREENING OF EDUCATIONAL AIDS ON PREVENTIVE HEALTHCARE IN LOCAL LANGUAGES
PHASE 1 :: MOBILE OUTREACH CENTERS CENTRAL INSTITUTE MOBILE CLINIC :: 3 MOBILE CLINIC :: 1 MOBILE CLINIC :: 2 EACH CLINIC WILL COVER ONE PLACE FOR 2 DAYS IN A WEEK CLINICS WILL BE WITHIN A DISTANCE OF 100-150 KMS FROM THE CENTRAL INSTITUTE
REPORTS OF THE DIAGNOSTIC TESTS TO BE DELIVERED TO THE OUTREACH CENTERS NEXT DAY. • PATIENTS REQUIRING FURTHER WORK-UP / HOSPITALIZATION TO BE REFERRED AND GUIDED TO THE MAIN HOSPITAL • AFTER 1 YEAR OF OPERATIONS, SET UP A TELEMEDICINE FACILITY IN THESE LOCATIONS CONNECTED TO MAIN HOSPITAL WHICH WILL OPERATE 7 DAYS/WEEK • MOBILE CLINICS TO CONTINUE 2 DAYS/WEEK • EXPAND THE SCOPE OF THESE CLINICS TO COVER A RADIUS OF 300 KMS IN NEXT 1 YEAR & GRADUALLY CONVERT THESE TO PERMANENT PERIPHERAL OUTREACH CLINICS EQUIPPED WITH BASIC FACILITIES AND HAVE AT LEAST 2 DOCTORS POSTED IN EACH CLINIC ON A ROTATION BASIS
IN PHASE II IDENTIFY 2-3 OUTREACH CENTERS WHICH CAN BE EXPANDED TO SMALL 20-30 BEDDED HOSPITALS MANNED BY DOCTORS TRAINED IN THE MAIN INSTITUTE AND EQUIPPED WITH ALL BASIC FACILITIES LIKE : • OPD FACILITIES • BASIC LABORATORY SERVICES • BASIC RADIOLOGY TESTS • 1 MAJOR OPERATION THEATRE • 1 MINOR OPERATION THEATRE • TELEMEDICINE FACILITIES • 2 - 4 BEDDED INTENSIVE CARE UNIT • ** Will explore the possibility of a tie-up with “the NGOs working in the rural level” to make the rural model more effective and at the same time involve them in a new field of social initiative
ALSO IN PHASE II • EXPANSION & ADDING OF NEW FACILITIES IN THE MAIN HOSPITAL AS PLANNED (EXPAND CAPACITY BY ANOTHER 150 – 200 BEDS WITH PROPORTIONATE INCREASE IN INTENSIVE CARE BEDS) • START AN INSTITUTE FOR PARA-MEDICAL ,NURSES TRAINING & HOSPITAL ADMINISTRATION IN TIE-UP WITH A REPUTED UNIVERSITY • START 2-3 CLINICS WITH DIAGNOSTIC CENTRES IN / AROUND GUWAHATI CITY OFFERING FACILITIES WITH CROSS-SUBSIDIZATION • ADD 1-2 MORE MOBILE CLINICS TO EXPAND THE SCOPE OF OUTREACH CLINICS TO INCLUDE AT LEAST 3-4 MORE PLACES
PHASE III • EXPANSION & ADDING OF NEW FACILITIES IN THE MAIN HOSPITAL AS PLANNED (EXPAND CAPACITY BY ANOTHER 150 - 200 BEDS WITH PROPORTIONATE INCREASE IN INTENSIVE CARE BEDS) • INTRODUCTION OF DNB, PDCC, FELLOWSHIP COURSES • IDENTIFY 2-3 MORE OUTREACH CENTERS WHICH CAN BE EXPANDED TO IDENTICAL SMALL HOSPITALS AS IN PHASE II
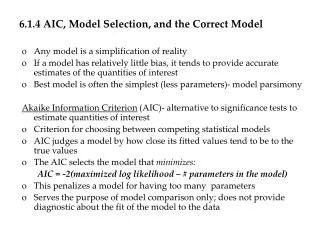
PHASE IV • EXPANSION & ADDING OF NEW FACILITIES IN THE MAIN HOSPITAL AS PLANNED (EXPAND CAPACITY BY ANOTHER 150 BEDS WITH PROPORTIONATE INCREASE IN INTENSIVE CARE BEDS) • CONTINUE THE PROCESS TILL WE CAN HAVE AT LEAST ONE 20-30 BED HOSPITAL UNIT IN DIFFERENT DISTRICTS OF ASSAM WITH 3 - 4 OUTREACH CENTERS MONITORED BY IT AND MAYBE 1 TELEMEDICINE CENTER IN EACH STATE OF NORTH EAST
OUTREACH HOSPITAL OUTREACH HOSPITAL CENTRAL INSTITUTE OUTREACH HOSPITAL OUTREACH HOSPITAL
IN SUMMARY TO CREATE A MODULAR HEALTHCARE DELIVERY SYSTEM WHICH WILL BE SELF SUSTAINABLE , EFFECTIVE & CAN TRULY INTEGRATE & DELIVER PRIMARY, SECONDARY & TERTIARY HEALTHCARE TO ALL SECTIONS OF THE SOCIETY AND TO CREATE A HEALTHCARE INSTITUTE WHICH IN THE NEXT 5-10 YEARS WILL BE COUNTED UPON AS AMONGST THE BEST MULTI-SPECIALTY INSTITUTES IN THE COUNTRY AND CAN ATTRACT PATIENTS FROM ALL OVER THE REGION AND CAN ALSO PLAY A PIVOTAL ROLE IN DEVELOPING MEDICAL TOURISM (take into consideration the New “Look East Policy”)