Download
1 / 26
260 likes | 339 Views
Kath Roberts Lifestyle Data. What do we mean by ‘lifestyle’? Why is local lifestyle data useful? Sources of lifestyle data and their comparative strengths and weaknesses. Lifestyle?. Smoking Physical activity Diet Alcohol consumption Use of drugs Sexual behaviour Obesity

E N D
What do we mean by ‘lifestyle’? • Why is local lifestyle data useful? • Sources of lifestyle data and their comparative strengths and weaknesses
Lifestyle? • Smoking • Physical activity • Diet • Alcohol consumption • Use of drugs • Sexual behaviour • Obesity • Sexually transmitted infections • Teenage pregnancy • Breastfeeding • Blood pressure • Cholesterol levels
Question What’s the best way to estimate the percentage of people in your local population who smoke?
Potential data sources • national surveys • synthetic estimates based on national surveys • local surveys • data from primary care • data from commercial/market research organisations
What do we really want to know? Which lifestyle factor? • Smoking • Physical Activity • Diet • Obesity • Alcohol consumption What ? • Between area comparisons • Within-area comparisons • Trends over time • Evaluating local services/initiatives
The need for local lifestyle data - general: • prioritising, planning, targeting and evaluating local services and lifestyle change initiatives • data at LA/PCT-level AND below for ... • comparison with other LAs/PCTs • within-area comparisons by age, gender, ethnicity, ward, practice, etc • analysis of trends over time and progress towards local targets • measuring the outcomes/impacts of services
The need for local lifestyle data - specific: • Local Operational Plans (LOPs) • based on the “Vital Signs” indicators • Local Area Agreement (LAAs) • based on the National Indicator Set (NIS) • Joint Strategic Needs Assessment (JSNA) Vital Signs and NIS lifestyle indicators include: • child obesity • smoking quitters • hospital admissions for alcohol-related harm • adult physical activity levels • school PE and sport provision • breastfeeding
The need for local lifestyle data (cont.) • helps to communicate important public health messages ... • ... to the public/local communities • ... to decision makers/commissioners/funders
Some criteria for assessing and comparing different sources • Validity • Reliability • Accuracy • Bias • Precision • Timeliness • Cost • Does it measure what it aims to measure? • Do questions produce reproducible answers? • Measurement or data entry? • Is the sample representative? • Adequate sample size?
Data from primary care • records of consultations held on practice computers • incentives - the QOF system • GP research databases
The Quality and Outcomes Framework (QOF) is a system of financial rewards to general practices for the provision of high quality care Obesity: The practice can produce a register of patients aged 16 years and over with a BMI greater than or equal to 30 in the last 15 months. Smoking 1: The percentage of patients with any or any combination of the following conditions: coronary heart disease, stroke or TIA, hypertension, diabetes, COPD or asthma whose notes record smoking status in the previous 15 months (except those who have never smoked where smoking status need only be recorded once since diagnosis). Smoking 2: Ditto ... but where the notes contain a record that smoking cessation advice or referral to a specialist service, where available, has been offered within the previous 15 months.
Data from primary care • Advantages • Standardised national systems. • Ongoing data collection • Established coding systems. • Disadvantages: • Selective focus on particular patient groups • Variability between practices in the completeness and quality of data recording. • Lack of a geographical focus
Data from commercial organisations • e.g. CACI, Claritas, Experian, Acxiom, Dr Foster • large volumes of household survey and consumer data modelled to provide estimates for all areas of the country of e.g.: • expenditure on tobacco, food and drink • prevalence of smoking and obesity
Acxiom smoking prevalence estimates Data from commercial organisations e.g. • based on the “National Shoppers Survey” • large national sample - some coverage in your area • updates available annually • adjusted for known biases in the sample e.g. undersampling of young people. • relatively cheap • 2005 data gave a national prevalence of 17% compared to 23-24% from 2004-5 GHS and 2004 HSE
Data from commercial organisations Advantages: • Extensive geographical coverage Disadvantages: • the main problem is that detailed methodologies are often not available • Potential for bias (lack of random sampling / poor response rates) • Cost – expensive?
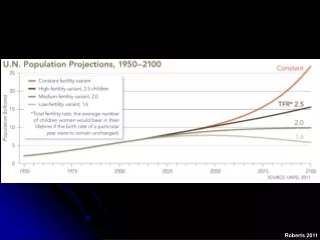
National surveys • Health Survey for England • General Household Survey / Integrated Household Survey • Smoking prevalence available at PCT level from 2010 • Smoking, drinking and drug use • Tellus National surveys are often not large enough to provide data below regional level – data aggregation / local boost samples may be options....
National surveys – local boosts Advantages • Flexibility. • Robust methodology. • Comparability with national, regional and other benchmarks. Disadvantages • Lack of local historical trend data. • Costs
Model-based estimates of healthy lifestyle • IC-funded project • HSfE 2003-2005 data on smoking, obesity, binge drinking, fruit and veg consumption • statistical modelling to identify social and demographic predictors of these aspects of lifestyle • LA- and MSOA-level estimates (and CIs) based on the social and demographic characteristics of their populations. • validated against other survey data, e.g. the Merseyside boost of the HSfE
Model-based estimates of healthy lifestyle Example: LA-level smoking model Area characteristics statistically associated with prevalence of smoking: • high % households with no car • low % of people 16-74, professional & managerial occupations • high % males, 16-34, White ethnic origin • low life expectancy (females) • low % with limiting long-term illness
Model-based estimates of healthy lifestyle Advantages • Comprehensive geographical coverage - allows comparative analysis between areas. • Ease of access/cost. The estimates are in the public domain, are immediately accessible to users and are free of charge. Disadvantages • Lack of flexibility – particular local requirements cannot be specified. • Lack of sensitivity to local lifestyle interventions. - represent expected prevalence so additional local factors that may impact true prevalence are not taken into account, so should not be used to measure change over time.
Local surveys (including regional surveys) Advantages: • generates real local data • flexibility and control over e.g.: • population to be surveyed - area, age, sex, ethnicity, etc • sample size - trading statistical power v cost • survey design - cross-sectional/longitudinal, census/sample, etc • method - phone, internet, interview, postal • subject matter - can be anything!!
Local surveys (including regional surveys) Disadvantages: • lack of standardisation of questions and derived indicators • lack of comparability with other areas/benchmarks • securing permissions • labour intensive • cost
smoking prevalence in your local authority area rate the different sources for different applications