Download
1 / 38
390 likes | 642 Views
DEGLUTITION REFLEX. DR AMNA TAHIR ASSISTANT PROFESSOR PHYSIOLOGY DEPARTMENT. Stages of Swallowing (Deglutition). Oral stage (voluntary) Pharyngeal stage Esophageal stage. Swallowing (Deglutition). Vagus & glossopharyngeal nerves for upper 1/3 Vagus nerve innervates the lower 2/3.

E N D
DEGLUTITION REFLEX DR AMNA TAHIR ASSISTANT PROFESSOR PHYSIOLOGY DEPARTMENT
Stages of Swallowing (Deglutition) • Oral stage (voluntary) • Pharyngeal stage • Esophageal stage
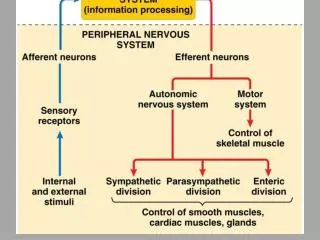
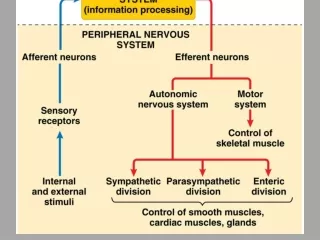
Swallowing (Deglutition) • Vagus & glossopharyngeal nerves for upper 1/3 • Vagus nerve innervates the lower 2/3
Swallowing (Deglutition) Brain Stem (medulla & pons) (swallowing center) CN V, IX, X & XII
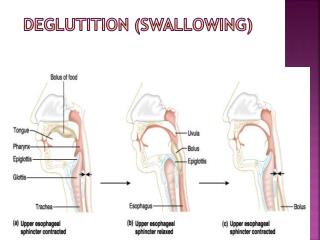
Swallowing (Deglution) Swallowing can be divided into: • Voluntary stage of swallowing • Bolus voluntarily squeezed or rolled posteriorly against the palate • Swallowing cannot be stopped • Pharyngeal stage of swallowing • Bolus reaches posterior mouth & pharynx stimulates receptors initiate series of automatic pharyngeal muscle contraction
Automatic pharyngeal muscle contraction: • Soft palate is pulled upward and prevents the reflux of food to nasal cavity • Palatopharyngeal folds are pulled medially to approximate each other – form a saggital slit • Vocal cords are approximated • Larynx is pulled upward & anterior by neck muscles • Epiglottis swing backward over the opening of larynx
Automatic pharyngeal muscle contraction: • Upward movement of larynx & enlargement the opening of esophagus • Upper 3-4cm of esophagus relaxes • Muscular wall of pharynx contracts to push the food downward (propulsive contraction) N.B. pharyngeal stage lasts for < 2 sec
Swallowing (Deglution) • Esophageal stage of swallowing • Conducts food rapidly to the stomach • Two types of peristaltic movements: • 1° peristalsis: – continuation of a peristaltic wave – begins in pharynx & spreads into esophagus – passes in 8-10 sec • 2° peristaltic waves: – results from the distention of esophagus – begins if the 1° wave failed to push the food down
Deglutition (Swallowing) Figure 22.13a-c
Receptive relaxation of stomach • As the waves of peristalsis pass thru esophagus to stomach, a wave of relaxation precedes the peristalsis, which transmitted thru myenteric inhibitory neurons
Function of lower esophageal sphincter (Gastroesophageal sphincter) • above the junction of esophagus with stomach by 3cm • remains tonically constricted • peristaltic swallowing wave passes down esophagus receptive relaxation of gastro-esophageal sphincter allow food go easily to stomach • Sphincter does not relax satisfactorily condition called achalasia
Esophageal reflux can be prevented by: • Gastro-esophageal sphincter • Valve-like mechanism: short portion of the esophagus that extends beneath the diaphragm before opening into stomach
Deglutition (Swallowing) Figure 22.13d, e
the factors that contribute to the competence and tone of the lower esophageal sphincter • Lower esophageal sphincter (LOS) is formed by the lowest 2 – 4cm segment of the esophagus • - Physiological sphincter • Resting pressure: 15 – 25mmHg (20 – 30 cmH2O) above gastric pressure Prevents reflux
- Barrier pressure = LOS P – intragastric P (10cmH2O @ rest) Normally Barrier P = 25cmH2O, reflux at <13cmH2O ↑intra-abdominal P (pregnancy) will ↑intragastric P → ↓barrier P
Neural Control • Internal relaxation- contraction cycling (smooth mm) coordinated by medulla via vagus • External portion of sphincter (crura) supplied by phrenic nerve
Factors contributing to competence/tone 1-Tonic contraction of circular muscle fibers 2-Oblique gastro-esphagealangle forms a mucosal flap-valve mechanism 3-Crura of diaphragm forms pinch-cock mechanism 4- LOS is intra-abdominal
- Enhances LOS tone with positive IAP rather than negative ITP -↑LOS tone with cough/sneeze 5. Hormones - ↑LOS tone: gastrin, motilin, α-adrenergic stimulation, oestrogen • - ↓LOS tone: secretin, glucagon, VIP, GIP,PROGESTONE
Gastro esophageal reflux Gastro esophageal reflux is a condition where the acidic content of the stomach regurgitates back into the esophagus. The distal esophageal mucosa is non glandular in type (it is squamous epithelium), therefore, it can easily be damaged by chronic acid reflux. -- TO prevent this, there are several mechanisms in place
The lower oesophageal sphincter (LOS) is tonically active but relaxes on swallowing. The tonic activity of the LOS between meals prevents reflux of gastric contents into the oesophagus. • The prominent smooth muscle of the lower oesophagus acts as a internal phincter to prevent reflux. • The right crus of the diaphragm which surrounds the oesophagus exerts a pinch-cock like action on the oesophagus to prevent reflux (external sphincter).
The oblique or sling fibers of the stomach wall create a flap valve that helps close off the esophago-gastric junction and prevent regurgitation when intra-gastric pressure rises. • Another factor that helps to prevent reflux is a valve like mechanism of a short portion of the esophagus that extends slightly into the stomach. Increased intra-abdominal pressure caves the esophagus inward at this point. Thus, this valve like closure of the lower esophagus helps to prevent high intra-abdominal pressure from forcing stomach contents backward into the esophagus
CAUSES OF DYSPHAGIA Oral( painful mastication) • Oral malignancy • Tonsillitis • Herpes simplex • Aphthous ulceration • stomatitis
Pharyngeal • Following cerebrovascular disease ( stroke) • Bulbar and pseudo bulbar palsy • Pharyngeal malignancy • Myasthenia gravis • Motor neuron disease • Pharyngeal diverticulum
esophagus Motility disorders • Achalasia • Diffuse spasm • Scleroderma
Extrinsic pressure • Mediastinal mass lesion • Bronchogenic carcinoma • Dilated left atrium • Aortic aneurysm • Foreign bodies • goitre
Intrinsic pressure • Benign esophageal stricture • Carcinoma • webs and rings • Lower esophageal ring
ACHALASIA CARDIA • It is a disease of an unknown etiology characterized by aperistalsis in the body of oesophagus and failure of relaxation of lower oesophageal sphincter on initiation of swallowng . • The food collects in capacious oesophagus resulting in dilatation of oesophagus
Clinical features • Dysphagia • Regurgitation • Retrosternal chest pain
Investigation • X-ray chest • Barium swallow • Oesophagoscoy
Treatment • Endoscopic • Pneumatic dilatation • Botulism • Surgical