Download
1 / 17
180 likes | 476 Views
Vorhofflimmern (FA). Sinusrhythmus (SR). Fehlendes P, Vorhofflimmernwellen (350-600/min), unregelmäßige RR-Intervalle. Vorhofflimmern - EKG. Vorhofflimmern - Epidemiologie. Generell 0,4 – 2% < 60a = < 1 %, >60a = 4 %, >80a = 10 % 1-1,5 % Zunahme / Dekade

E N D
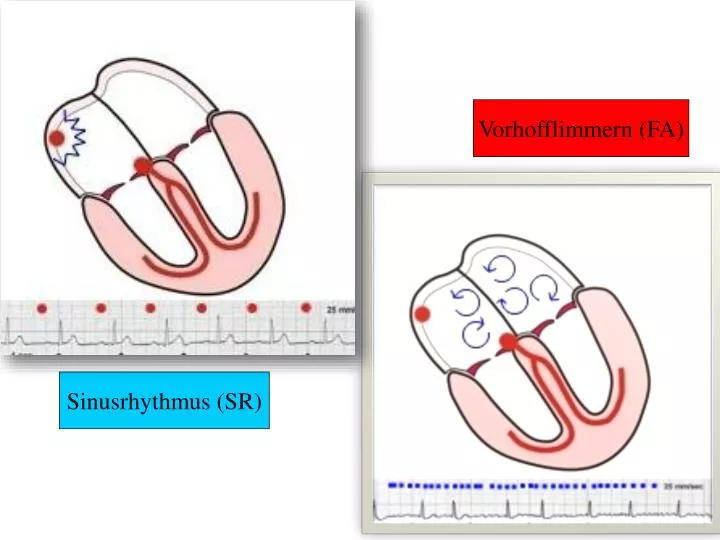
Vorhofflimmern (FA) Sinusrhythmus (SR)
Fehlendes P, Vorhofflimmernwellen (350-600/min), unregelmäßige RR-Intervalle Vorhofflimmern - EKG
Vorhofflimmern - Epidemiologie • Generell 0,4 – 2% • < 60a = <1 %, >60a = 4 %, >80a = 10 % • 1-1,5 % Zunahme / Dekade • Medianes Alter 75a, 70 % zwischen 65-85a • >40a = 1:4 Risiko für AF • Männer > Frauen • Europa 6 Mill., EU 4,5 Mill., USA 2,5 Mill.BRD 1 Mill., Österreich 120.000 Menschen • Jährliche Kosten: 3.000 Euro/Patient
Prognose - Bedeutung • Sterblichkeit: x 2, Herzschwäche: x 3, Schlaganfall: x 5, Lebensqualität: x ?? • FA verantwortlich für 15% aller Schlaganfälle • Risiko Schlaganfall bei FA und >80a: 23,5% • FA bei Schlaganfall verdoppelt Todesrate • Schlaganfall • 10% aller Todesursachen • 85% ischämisch, 15% hämorrhagisch • Morbidität 50% nach 1a, 88% der Kosten extramural
Vorhofflimmern - Ursachen • Hochdruck • Koronare Herzkrankheit • Herzschwäche • Herzklappenfehler • Entzündliche und infiltrative Herzerkrankungen • Herztumore • Postoperativ (Herz-, Lungen-, Speiseröhrenoperationen) • Angeborene Herzerkrankungen • Familiär • Hyperthyreose, Phäochromozytom • Alkohol • Idiopathisch (‚lone atrial fibrillation‘) 12-30%
AFib-Guidelines der ESC 2010 FA – erstmals diagnostiziert stumm? paroxysmal (<48h) persistierend (CV nötig) rezidivierend langdauernd (>1a) permanent (akzeptiert) chronisch
AFib-Guidelines der ESC 2010 FA - Symptome EHRA = European Heart Rhythm Association Welche? Herzunruhe („Palpitation“; paroxysmal>), Schwindel, Atemnot (permanent>)
Kardioversion oder Antikoagulation Rhythmuskontrolle Frequenzkontrolle
RHYTHMUS Kardioversion Elektrisch (biphasisch>), pharmakologisch (Vernakalant, Propafenon ..) Rezidivprophylaxe BIG 5:Amiodaron, Dronedaron, Flecainid, Propafenon, Sotalol Ablationparoxysmal > permanentFA danach oft asymptomatisch Maze-Operation AtrialerDefibrillator Spezielle Stimulationstechniken FREQUENZ Medikamente Digitalis (inaktive Pat.>), Verapamil, ß-Blocker Amiodaron, Dronedaron (nicht: NYHA III und IV) MILD (<110/min versus STRINGENT (<80/min) – asymptomatisch ! AV-Knoten-Ablation mit Schrittmacherimplantation AV-Knoten-Modifikation seit 1962
FA – „Pill-in-the-Pocket“-Konzept • Aus Italien • Indikation • herzgesunde Patienten • paroxysmale FA • deutlich symptomatisch, maximal 2-3/Monat • Erfolgsquote bis 90% • Propafenon (bis 600mg) 5 min nach Beginn • Liegende / sitzende Körperhaltung • Selbstkontrolle: Bradykardie, Tacharrhythmie, Dyspnoe, Prä-/Synkope • Arztkontakt: FA > 8h oder bei NW • Weiters: Valsalva-Manöver (Anpressen, Trinken, Carotis-, Bulbusmassage), Wait-over-Night (+ gering Alkohol / Schlaftablette)
FA – „Upstream“-Therapie • RAAS-Blockeratrialer Druck , Suppression der atrialen Fibrose, Inflammation , Hemmung des elektrischen Remodelings • ACE-Hemmer • Angiotensinrezeptorblocker • Aldosteronantagonisten • Statineantiinflammatorisch, antioxidativ, NO-Endothelfunktion, Downregulation RAS; Plaquestabilisierung, autonomes NS • Mehrfach ungesättigte Fettsäuren • Fischkost • Gewichtskontrolle
CHA2DS2-VASc-Score maximal 9 Punkte
HAS-BLED-Score maximal 9 Punkte
AF – Schlaganfall / Thrombembolie • Aspirin 325mg/d, wenn CHADS2-Score niedrig • Clopidogrel + ASS bringt nichts • Antikoagulation • 6 randomisierte Studien (AFASAK, SPAF, BAATAF, CAFA, SPINAF, EAFT) – 64% Reduktion des Schlaganfalls [Exklusionsrate sehr hoch] • MarcoumarR Internist, SintromR Chirurg • geschätzt nur für 30-60% • bis zu 30% abgesetzt nach 1 Jahr • INR-korrekt um 40% • Perkutaner Verschluss linkes Herzohr
UFH, LMWH, Fondaparinux Rivaroxaban Apixaban Dabigatran