Download
1 / 1
10 likes | 138 Views
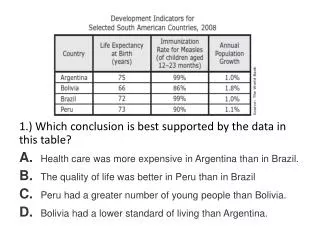
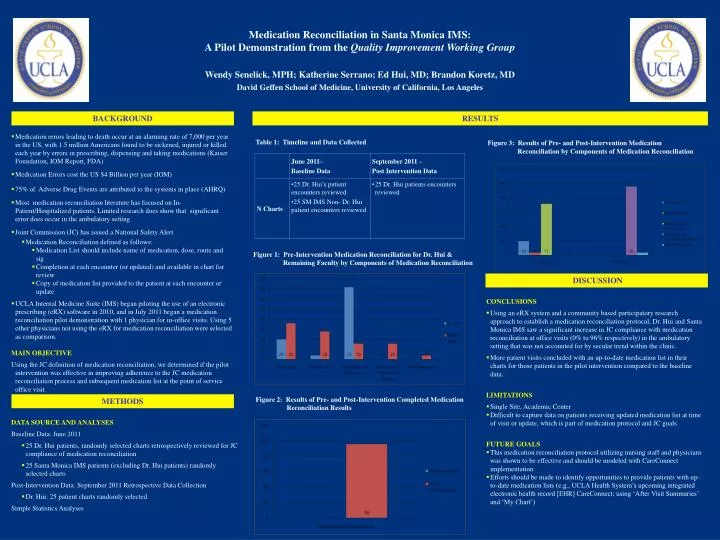
Medication Reconciliation in Santa Monica IMS: A Pilot Demonstration from the Quality Improvement Working Group. Wendy Senelick, MPH; Katherine Serrano; Ed Hui, MD; Brandon Koretz, MD David Geffen School of Medicine, University of California, Los Angeles. BACKGROUND. RESULTS. METHODS.

E N D
Medication Reconciliation in Santa Monica IMS: A Pilot Demonstration from the Quality Improvement Working Group Wendy Senelick, MPH; Katherine Serrano; Ed Hui, MD; Brandon Koretz, MD David Geffen School of Medicine, University of California, Los Angeles BACKGROUND RESULTS METHODS DISCUSSION • Medication errors leading to death occur at an alarming rate of 7,000 per year in the US, with 1.5 million Americans found to be sickened, injured or killed each year by errors in prescribing, dispensing and taking medications (Kaiser Foundation, IOM Report, FDA) • Medication Errors cost the US $4 Billion per year (IOM) • 75% of Adverse Drug Events are attributed to the systems in place (AHRQ) • Most medication reconciliation literature has focused on In-Patient/Hospitalized patients. Limited research does show that significant error does occur in the ambulatory setting • Joint Commission (JC) has issued a National Safety Alert • Medication Reconciliation defined as follows: • Medication List should include name of medication, dose, route and sig • Completion at each encounter (or updated) and available in chart for review • Copy of medication list provided to the patient at each encounter or update • UCLA Internal Medicine Suite (IMS) began piloting the use of an electronic prescribing (eRX) software in 2010, and in July 2011 began a medication reconciliation pilot demonstration with 1 physician for in-office visits. Using 5 other physicians not using the eRX for medication reconciliation were selected as comparison. • MAIN OBJECTIVE • Using the JC definition of medication reconciliation, we determined if the pilot intervention was effective in improving adherence to the JC medication reconciliation process and subsequent medication list at the point of service office visit. Table 1: Timeline and Data Collected Figure 3: Results of Pre- and Post-Intervention Medication Reconciliation by Components of Medication Reconciliation Figure 1: Pre-Intervention Medication Reconciliation for Dr. Hui & Remaining Faculty by Components of Medication Reconciliation • CONCLUSIONS • Using an eRX system and a community based participatory research approach to establish a medication reconciliation protocol, Dr. Hui and Santa Monica IMS saw a significant increase in JC compliance with medication reconciliation at office visits (0% to 96% respectively) in the ambulatory setting that was not accounted for by secular trend within the clinic. • More patient visits concluded with an up-to-date medication list in their charts for those patients in the pilot intervention compared to the baseline data. • LIMITATIONS • Single Site, Academic Center • Difficult to capture data on patients receiving updated medication list at time of visit or update, which is part of medication protocol and JC goals • FUTURE GOALS • This medication reconciliation protocol utilizing nursing staff and physicians was shown to be effective and should be modeled with CareConnect implementation. • Efforts should be made to identify opportunities to provide patients with up-to-date medication lists (e.g., UCLA Health System’s upcoming integrated electronic health record [EHR] CareConnect; using ‘After Visit Summaries’ and ‘My Chart’) Figure 2: Results of Pre- and Post-Intervention Completed Medication Reconciliation Results • DATA SOURCE AND ANALYSES • Baseline Data: June 2011 • 25 Dr. Hui patients, randomly selected charts retrospectively reviewed for JC compliance of medication reconciliation • 25 Santa Monica IMS patients (excluding Dr. Hui patients) randomly selected charts Post-Intervention Data: September 2011 Retrospective Data Collection • Dr. Hui: 25 patient charts randomly selected • Simple Statistics Analyses