Download
1 / 74
740 likes | 873 Views
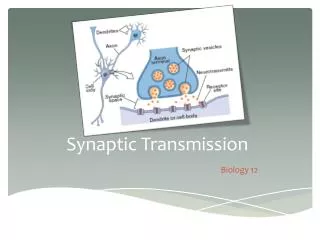
Review sequence of events involved in synaptic transmission Ch. 4 (cont’d). Verbal description and animation (shown in class). Neurotransmitters and Receptors Ch. 4 (cont’d). Amino Acid Neurotransmitters.

E N D
Review sequence of events involved in synaptic transmissionCh. 4 (cont’d)
Amino Acid Neurotransmitters • Amino acids are the building blocks of all proteins in the body; they can serve as fast-acting, point-to-point synapses • There is conclusive evidence that glutamate, aspartate, glycine, and gamma-aminobutyric acid (GABA) are neurotransmitters • They come from proteins we eat
Monoamine Neurotransmitters • Monoamine neurotransmitters are formed by slight modification to amino acid molecules • They are often released from string-of-bead axons, and they have slow lingering, diffuse effects; neurons that release monoamines typically have their cell bodies in the brain stem
Monoamine Neurotransmitters • There are four monoamine neurotransmitters and they belong to one of two subclasses: • Catecholamine neurotransmitters: dopamine, norepinephrine, epinephrine; all three are sythesized from amino acid tyrosine Tyrosine -> L-DOPA -> dopamine -> norepinephrine -> epinephrine
Monoamine Neurotransmitters • Indolamine neurotransmitter: serotonin; synthesized from the amino acid tryptophan
Acetylcholine • ACh is the small molecule transmitter at neuromuscular junctions (where neuron meets muscle cell) at many synapses in the ANS, and at CNS synapses; • ACh is the only neurotransmitter known to be deactivated in the synapse by enzymatic degradation rather than by uptake; it is deactivated by an enzyme acetylcholinesterase
Neuropeptide Transmitters • Peptides are short chains of 10 or fewer amino acids; over 50 peptides are putative neurotransmitters; They are the largest neurotransmitters • Endorphins are an example of a neuropeptide transmitter; they are opiate-like transmitters that are important to analgesia and reward systems in the brain
Soluble Gas Neurotransmitters • This class of recently identified neurotransmitters include nitric oxide and carbon monoxide • The gasses are produced in the neural cytoplasm, diffuse immediately through cell membrane into the extracellular fluid and into nearby cells to stimulate production of second messengers • They are difficult to study as they act rapidly and are immediately broken down, existing for only a few seconds
Extra credit question • (drawing on white board in class)
Pharmacology ofSynaptic Transmission • Drugs that facilitate a transmitter’s effects are called agonists; drugs that reduce a transmitter’s effect are called antagonists • Drugs act upon one or more of the steps in neurotransmitter action; the exact mechanism varies from drug to drug
Pharmacology ofSynaptic Transmission • For example, cocaine is a catecholamine agonist that acts by blocking the reuptake of dopamine and norepinephrine
Pharmacology ofSynaptic Transmission • By contrast, valium is a GABA agonist that acts by increasing the binding of GABA to its receptor • GABA is an inhibitory neurotransmitter (it’s receptor allows Cl- in, hyperpolarizing, IPSPs)
Pharmacology ofSynaptic Transmission • Atropine and curare are both ACh antagonists; • atropine blocks muscarine receptors, not allowing acetylcholine to bind • whereas curare paralyzes by blocking nicotinic receptors, not allowing acetylcholine to bind
Principles of Drug Action Ch. 15
Outline • Drug administration • Drug Tolerance • Addiction • Commonly Abused Drugs
Ingestion • Once swallowed drugs dissolve in the stomach fluids and are carried to the intestine where they are absorbed into the bloodstream • Cross blood-brain barrier
Injection • Subcutaneous, intramuscular, or intraveneous injections of drugs to get to blood stream • Cross blood-brain barrier
Inhalation • Drugs are absorbed into the capillaries of the lungs • Cross blood-brain barrier
Absorption through Mucous Membranes • Absorbed by mucous membranes in nose, mouth, or rectum, gets into bloodstream • Crosses blood-brain barrier
Drug tolerance • State of decreased sensitivity to a drug that develops as a result of exposure to it
Cross Tolerance • Exposure to one drug can produce tolerance to other drugs that act by the same mechanism
Metabolic Tolerance • Type of drug tolerance that results from changes that reduce the amount of the drug getting to its site of action
Functional Tolerance • Drug tolerance that results from changes that reduce the reactivity of the sites of action to the drug
Physical Dependence • If an individual suffers from withdrawal symptoms they are physically dependent on that drug • Withdrawal syndrome is when an adverse physiological reaction results from sudden elimination of the drug
Addiction • An individual is considered an addict if they are habitual drug users who continue to use drugs despite its adverse effects on their health, social life, and despite repeated attempts to stop using it
Common Drugs • Tobacco • Alcohol • Marijuana • Cocaine and amphetamine • MDMA (Ecstasy) • The Opiates
Tobacco • Active ingredient - nicotine • Highly physically addictive • Acts on nicotinic receptors
Alcohol • Alcohol is a depressant - it reduces neural firing by reducing the flow of Ca++ ions into neurons by acting on ion channels, and thus not releasing as many vessicles with neurotransmitter (many kinds) into the synapse (antagonistic) • Also is agonistic, increasing the binding of GABA to its receptor
Alcohol • Highly physically addictive - strong physical dependence, physical withdrawal is “hangover” • Associated with Korsakoff’s syndrome - severe memory loss, sensory and motor dysfunction, and demetia due to malnutrition (lack of thiamine)
Marijuana • Cannabis sativa - active ingredient is THC • THC mimics endogenous chemical anandomide and binds to cannibinoid receptors
Marijuana • Effects are increased sense of well-being, the “giggles”, increased appetite, short-term memory problems, and difficulty with motor coordination and sequencing of events, and poor judgment
Marijuana • Brain areas involved are basal ganglia and cerebellum (both involved with motor coordination and sequencing of events), hippocampus (short term memory), and neocortex
Cocaine and Amphetamine • Stimulants that elicit feelings of overconfidence, alertness, energy, and friendliness • High doses can induce cocaine psychosis (or amphetamine psychosis) in which the individual shows symptoms similar to that of schizophrenics
Cocaine and Amphetamine • Highly psychologically addictive but low physical addiction (mild withdrawal symptoms)
MDMA (Ecstasy) • Agonistic effects on serontonergic and dopaminergic receptors • Targets terminal buttons and releases all of stored supply of vessicles containing serotonin • The synapses are flooded with serotonin
MDMA (Ecstasy) • Not clear what long-term effects are • “Suicide Tuesday” • So far, individuals exhibit severe changes in serotonergic function, and mood problems, memory deficits, and motor problems • Mainly affects frontal lobe (reasoning, motor) and hippocampus (memory)
MDMA (Ecstasy) • Study on monkeys who were given Ecstasy twice a day for four days • Short-term damage (upon taking pill) • Long-term damage (two weeks after first day)
MDMA (Ecstasy) • Damage still observed seven years later (!), but less severe
Opiates • Heroin, morphine, and codeine are all opiates • Used mainly as analgesics (pain killers) but are addictive
Outline • Theories of Addiction a. Physical-Dependence Theories b. Positive-Incentive Theories (2) Intracranial Self-Stimulation (ICSS) a. Mesotelencephalon Dopamine System (3) Neural Mechanisms of Motivation and Addiction
Critical Question • Do addicts abuse a drug because they are trying to fulfill an internal need, or are they drawn by the anticipated positive effect of the drug?
Physical-DependenceTheories of Addiction • Early attempts to explain addiction attributed it to physical dependence; addicts take drugs to curtail the withdrawal symptoms that they otherwise would face • From this perspective, treating addiction meant withdrawal from the drug in a hospital setting until the symptoms subsided
Physical-DependenceTheories of Addiction • Unfortunately, addicts almost always return to drug taking after they have been released from the hospital • The failure of this treatment approach is not surprising in the light of two well-established facts about taking drugs:
Physical-DependenceTheories of Addiction • Some highly addictive drugs produce little withdrawal distress (e.g., cocaine) • The pattern of drug taking in many addicts typically involves self-imposed cycles of binges and detoxification
Physical-DependenceTheories of Addiction • Modern physical-dependence theories of addiction attempt to account for the inevitability of relapse after detoxification by postulating that withdrawal effects can be conditioned (meaning that if drug-free, they return to a situation where they once did drugs, they will have withdrawal effects opposite to the effects of the drug)
Physical-DependenceTheories of Addiction • There are two problems with this theory: • Many of the conditioned effects elicited by drug-taking environments are similar to the effects of the drug, not to the drug’s withdrawal effects • Addicts and experimental animals often find drug-related cues rewarding, even in the absence of the drug (e.g., “needle freaks” enjoy excitement of sticking empty hypodermic needles in their arms)