Download

1 / 41
750 likes | 2.18k Views
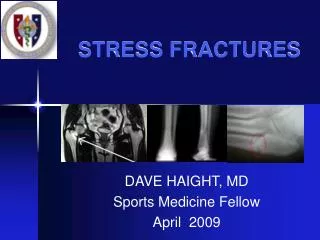
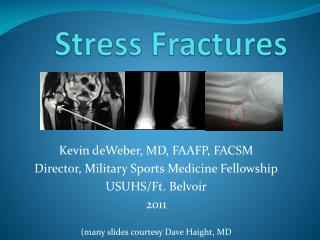
Stress Fractures. Locate the most common locations for Stress fractures. Frequency. Metatarsal(42) Tibia(36) Fibula(30) Navicular (26). Who is this person?. What injury just occurred?. Locate it. Overuse Injury.

E N D
Frequency Metatarsal(42) Tibia(36) Fibula(30) Navicular(26)
What injury just occurred? Locate it
Overuse Injury • Stress fractures represent one of the most common and potentially serious overuse injuries .The first cited reports on stress fracture were case studies of soldiers incurring such fractures in the 19th and early 20th centuries
History • People with stress fractures typically appear for treatment complaining of localized pain that gradually worsens, most commonly in the lower extremity. • Patients give a history of pain that is aggravated by physical activity and relieved by rest. • They usually recount a history of a recent increase in physical activity or the beginning of a new activity or some other change in their routine. • Palpation elicits localized tenderness over bone. • Additionally, swelling and erythema may be observed. If positive, radiographs are
Prevalence of Stress fracture • Stress fractures commonly occur in sedentary people who suddenly undertake a burst of exercise (whose bones are not used to the task). • They may also occur in Olympic-class athletes who do extraordinary quantities of high-impact exercise, in professional and amateur distance runners who run high weekly mileage, or in soldiers who march long distances.
Incidence • The civilian sports medicine literature reports stress fractures occurring during a wide variety of sport or exercise activities, such as running, fitness classes, basketball, baseball, volleyball, soccer, dancing, orienteering, and other activities • Running, however, appears to be the most commonly reported sport or exercise activity associated with the occurrence of stress fracture • Stress fractures account for 4–16 percent of running injuries . • The tibia, the most common site, accounts for 41–55 percent of stress fractures in most large case series.
Symptoms of a Stress fracture • Stress fractures usually have only a few symptoms. • A stress fracture could present as a generalized area of pain and tenderness associated with weight bearing. • Usually when running, a stress fracture in the leg or foot will cause severe pain at the beginning of the run, moderate pain in the middle of the run, and severe pain at the end and after the run.
How do stress fractures start? Causes?
Start? • Insidious onset of activity related pain • multifactorial
Wolff’s Law • Bone develops the structure most suited to resist the forces acting on it
Pathophysiology • underlying pathophysiology is believed to relate to repetitive mechanical loading of bone secondary to physical activity that stimulates an incomplete remodeling response . • According to this view, stress fractures occur when the early stage of remodeling, osteoclasticresorption of bone, outstrips the osteoblastic formation of new bone, resulting in a weakened bone that is vulnerable to injury.
Etiology of a Stress fracture • Bones are constantly attempting to remodel and repair themselves, especially during a sport where extraordinary stress is applied to the bone. • Over time, if enough stress is placed on the bone that it exhausts the capacity of the bone to remodel, a weakened site—a stress fracture—on the bone may appear. The fracture does not appear suddenly. • It occurs from repeated traumas, none of which is sufficient to cause a sudden break, but which, when added together, overwhelm the osteoblasts that remodel the bone.
Risk Factors • Previous stress fractures have been identified as a risk factor. • 60 % of athlete who sustain a stress fx had one previously
Female Triage • Eating disorder • Amenorrhea • Osteoporosis
Risk Factors • Studies of female runners with amenorrhea and irregular menses have shown greater risks of stress fracture. • A retrospective review of medical records for 207 female collegiate athletes found that women with a history of menstrual irregularity experienced an incidence of stress fracture 3.3 times higher than that of women with regular menses
Fitness is a risk factor • Studies of US military recruits have consistently shown significant associations between low aerobic fitness levels and higher risk of stress fracture during basic training • A study of 1,078 Marine recruits found that lower aerobic had an increase number of stress fractures
Why fitness important? • In a runner, each stride normally exerts large forces at various points in the legs. Each shock—a rapid acceleration and energy transfer—must be absorbed. • Both muscles and bones serve as shock absorbers. • However, the muscles, usually those in the lower leg, become fatigued after running a long distance and lose their ability to absorb shock. • As the bones now experience larger stresses, this increases the risk of fracture.
Race…..Why? • survey of female collegiate distance runners documented that White runners had a higher career prevalence of stress fractures diagnosed by radiograph or bone scan—a prevalence that was 2.4 times higher than that of Black runners
X-rays • Radiographic findings may include early lucent zones, periosteal new bone formation, focal sclerosis, endosteal callous, or later fractures or cortical cracks. • At the onset of symptoms, radiographs may be negative, and radiologic signs, if they become evident, may take several weeks to evolve. • While they are very specific, radiographs are not sensitive. Bone scans, on the other hand, are very sensitive
Diagnoses • X-ray on bone positive 2 to 10 weeks after injury
X-rays • radiographs were positive in only 14–53 percent of suspected cases, while 7–50 percent had neither positive bone scans nor radiographs.
X-rays • A study of 250 Marine recruits with lower extremity pain found that 54 percent of 839 clinically symptomatic scintigraphic abnormalities became radiographically positive 2–6 weeks after positive bone scans
Treatment • Early detection, Rest and Immobilization are key to best treatment. • Typical stress fracture healing time is 6-8 weeks for most sites. • The Tibia can take as much as 6-16 months. • Typically the fibula will heal in 6-12 weeks. The • Navicularwill usually take as much as 12 weeks or more and may require fixation. • The 5th Metatarsal will take 6 weeks or longer with weightbearing. As for the other lesser • Metatarsals, the 2nd Metatarsal usually takes 4-6 weeks, • while the 3rd and 4th Metatarsals take 4 weeks.
Treatment • usually includes muscle strength training to help dissipate the forces transmitted to the bones. • Bracing or casting the limb with a hard plastic boot or air cast may also prove beneficial by taking some stress off the stress fracture. An air cast has pre-inflated cells that put light pressure on the bone, which promotes healing by increasing blood flow to the area. This also reduces pain because of the pressure applied to the bone. If the stress fracture of the leg or foot is severe enough, crutches can help by removing stress from the bone. • With severe stress fractures, surgery may be needed for proper healing. The procedure may involve pinning the fracture site, and rehabilitation can take up to a half year.
Treatment • Strengthening exercises also help build muscle strength in the legs. • Strengthening these muscles will prevent them from becoming fatigued quickly, allowing them to absorb the strain of running for longer periods of time. • Key muscles that need strengthening with lower leg stress fractures are the calves and the shin muscles.
Prevention • Strategies designed to prevent stress fracture are not well understood. • Proposed strategies include gradual progressive initiation of vigorous physical training ,recovery periods with no running or marching after 2–3 weeks of training, use of proper running shoes , use of shock-absorbent insoles, use of orthotic shoe inserts, adherence to an appropriate diet, and treatment of abnormal menses.
Prevention • One method of avoiding stress fractures is to add more stress to the bones. • Though this may seem counter-intuitive (because stress fractures are caused by too much stress on the bone), moderate stress applied to the bone in a controlled manner can strengthen the bone and make it less susceptible to a stress fracture. • An easy way to do this is to follow the runner's rule of increasing distance by no more than 10 percent per week. This allows the bones to adapt to the added stress so they are able to withstand greater stress in the future.
Running • Depending on a variety of factors (including weight, running surface and shoe durability), runners should replace their shoes every 300–700 miles to allow adequate mid-sole cushioning. • A change in running surfaces can also help prevent stress fractures. • However, it is also argued that cushioning in shoes actually causes more stress by reducing the body's natural shock-absorbing action, increasing the frequency of running injuries.[6]
Pars interarticularis stress fracture spondylolysis • Repetitive hyperextension • Trunk rotation • Axial loading • 17% rowers • 14% gymnasts • 13% weightlifters • 27% throwing events in track
Pars Interarticularis Stress fracture • Pain hyperextension
Femoral stress fractures Do another time IR pain on PROM