Download
1 / 41
410 likes | 616 Views
You Can Control Your Asthma. Is it asthma ?. Saleh Alharbi MBBS FAAP FCCP ABP SBP Assistant Professor of Pediatrics Omm Al- Qura University Pediatric Pulmonologist, DSFH. Is it asthma? Acute care setting.

E N D
Is it asthma? Saleh AlharbiMBBS FAAP FCCP ABP SBP Assistant Professor of Pediatrics Omm Al-Qura University Pediatric Pulmonologist, DSFH
Is it asthma?Acute care setting • 3 m.o. child. Acute wheezing illness. No response to salbutamol. • 12 m.o. child. Acute wheezing illness. 3nd wheezing episode. Good response to salbutamol. • 4 y.o. girl. 1st episode of wheezing. Good response to salbutamol. • 2 y.o. boy. 1st episode. Severe wheezing. Poor response to salbutamol. Good response to oral steroids.
New patient SALMA is 36 months old girl • 6 “bronchitis” in year treated with antibiotics • 2 pneumonia • At last ED visit, Tx: • Fluxotide 125 2 puffs twice daily for 4 wks • Ventolin 2 puffs q 4 hrs as needed • Prednisone x 5 days
Is it asthma? Differential/co-morbidity? What type of asthma? Best management? What do you do?
What do you do?Elements to consider • Is itasthma?
What do you do?Elements to consider • Is it asthma? • Differential diagnosis / co-morbidity
Clinical clues to alternative diagnosis • Persistent moist cough • Excessive vomiting • Dysphagia • Abnormal voice or cry • Inspiratorystridor • Focal signs in chest • Finger clubbing • Failure to thrive • Cystic fibrosis; bronchiectasis; protracted bronchitis; aspiration; immune disorder; ciliarydyskinesia • Gastro-oesophageal reflux± aspiration • Swallowing problems (± aspiration) • Tracheal or laryngeal disorder • Laryngeal problem • Developmental anomaly; bronchiectasis; tuberculosis • Cystic fibrosis; bronchiectasis • Cystic fibrosis; immune disorder GINA: www.ginasthma.org
What do you do?Elements to consider • Is itasthma? • Differentialdiagnosis / co-morbidity • Review CXR • IgG, IgM, IgA • Sweat test
10% of children have diagnosed asthma 20% of children have asthma symptoms Asthma is the most prevalent chronic disease of childhood
Is it asthma? Differential/co-morbidity? What type of asthma? Best management? What do you do?
URTI URTI URTI TransientWheezing
Phenotypes & Evolution • Transient wheezing • before 2-3 yrs • No wheeze >3 yrs • Nonatopic wheezing • Trigger=URTI • Remit later in childhood (6 yrs) • Persistent wheeze • Atopy, IgE, eosinophils • Allergen sensitization<3yrs • Parental allergy • Severe intermittent wheezing • Well between URTI • Atopy, IgE, eosinophils • Transient early wheezing • Prematurity/parental smoking • No wheeze >3 yrs • Persistent early-onset wheezing (before age 3 yrs). • Trigger=URTI • No atopy/family atopy • Symptoms until at age 12 yrs • Late-onset wheezing/asthma. • Symptoms persist to adulthood • Atopy, IgE, eosinophils GINA: www.ginasthma.org. Practall. Allergy 2008: 63: 5–34
PRACTALL Consensus Report Identification of Asthma Phenotypes Is Critical Asthma Phenotypes in Children >2 Years of Age Is the child completely well between symptomatic periods? Yes No Are colds the most common precipitating factor? Is exercise the most common or only precipitating factor? Does the child have clinically relevant allergic sensitization? No No Yes Yes Yes No Virus-inducedasthmaa Exercise-inducedasthmaa Allergen-inducedasthma Unresolvedasthmaa,b aChildren may also be atopic. bDifferent etiologies, including irritant exposure and as-yet not evident allergies, may be included here. Adapted from Bacharier LB, et al. Allergy. 2008;63(1):5–34.
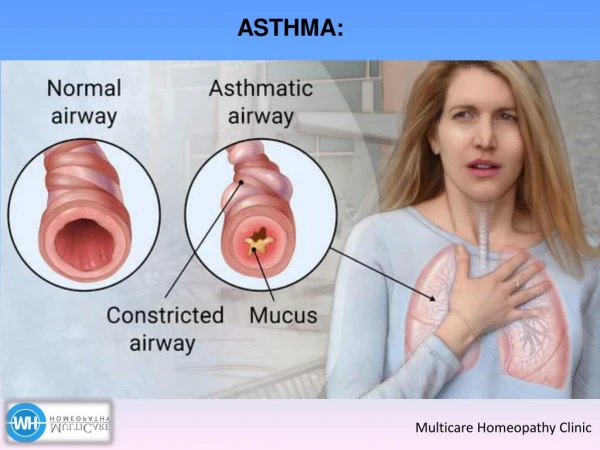
IS IT ASTHMA? Making the diagnosis of asthma may be difficult. Asthma may be considered if the following symptoms occur: • Recurrent episodes of wheezing. • Troublesome cough at night. • Cough, wheeze or shortness of breath after exercise. • Cough, wheeze or chest tightness after exposure to airborne allergens or pollutants. • Colds “go to the chest” or take more than 10 days to clear.
Natural history of asthma ASTHMA EXACERBATION ASTHMA FREE PERIOD REMISSION SYMPTOMS dry cough feeling of chest tightness audible musical wheezing increased work of breathing difficulties in walking, even talking duration - minutes, hours, days the expectoration of viscous sputum CLINICAL MANIFESTATION
ONSET: • acute or insidious • SIGNS • sitting position, leaning forward using the arms • paleness, cyanosis • sweat • hyperinflation of the chest • tachypnoe, tachycardia • pulsus paradoxus - reduction in pulse volume during inspiration • use of accessory muscles of respiration • increased percussion note • auscultation: prolonged expiration, wheezing, rhonchi, silent lung • barrel chest deformity, Harrison sulci, clubbing of the fingers
ASTHMA IN EARLY LIFEINFANTILE ASTHMA • significant number of asthmatic children demonstrates first obstructive episodes early in life • 30% < 1yr of age • 50-55% < 2 yr of age • 80% < 5 yr of age
Onset of Symptoms inChildren With Asthma 20% 30% 1-2 years <1 year 20% 2-3 years 30% >3 years McNicol and Williams. BMJ 1973;4:7-11; Wainwright et al. Med J Aust 1997;167:218-222.
Infantile asthma - criteria of diagnosis • 3 wheezy episodes (independent of atopy) • 2 wheezy episodes with atopic background (positive family or individual history) • 1 wheezy episode induced by exposure to allergen GINA recommendation • recurrent wheezing (wheezy bronchitis) other causes excluded positive response to therapy
DIAGNOSIS OF ASTHMA
The diagnosis of asthma has to be based largely on: Clinical judgment: History Symptoms physical findings In children 5 yearsand younger
Is it asthma? Obstruction, reversibility, hyper reactivity History Physical exam Laboratory Intense prolonged cough with URTIs “Bronchitis”: poor response to AB Good response to asthma Rx Signs of Obstruction Reversibility with ß2-agonists None
In children 5 yearsand younger Trial of treatment with SABA and ICS • Marked clinical improvement during the treatment • And deterioration when it is stopped • Supports a diagnosis of asthma
1. Case history • characteristics of asthma episode, frequency, duration, severity • types of triggers (precipitating, agravating) • the onset of the disease • atopic history • environmental history • previous and current therapy • response to medication • impact of disease on child, family, school attendence • psychosocial evaluation of patient/family • general medical history of child 2. Physical examination
In children over 5 yearsand olderPeak expiratory flow monitoring PFM is useful to establish diurnal variationand the severity of obstruction
3. lung function tests • considerable (more than 20%) variabilty of peak flow rate or FEV1 over short period of time daily variability= • response to bronchodilator when obstruction (improvement of at least 15-20% in PEF or FEV1) • measurement of bronchial hyperresponsiveness (decreasing of at least 15-20% in PEF or FEV1 after non-specific provocation) • basic spirometry - assessment of degree of obstruction PEF evening - PEF morning x 100 1/2 (PEF even. + PEF morn.)
3. Provocation studies: (a) Exercise: A 15% drop in FEV1 post exercise • indicates exercise induced asthma. (b) Metacholine challenge: A 20% reduction in • FEV1 at Metacholine concentrations < 8mg/ml • indicates bronchial hyperreactivity. • This is expressed as a PC20 value of eg 0.5mg/ml (= a20% reduction in FEV1 at 0.5mg/ml Metacholine).
4. assessment of allergy • SERUM IgE • measure of the allergy predisposition and their degree • the concentration is age dependent • total concentration • specific IgE level - against specific antigens; not more sensitive than skin test, results independent of therapy, skin lesions, dermographism, no risk of excessive (allergic/anaphylactic) reaction • normal values does not exclude allergy
4. assessment of allergy • SKIN TESTS • background - recovery of IgE on the surface of patient mast cells; interaction between allergen and IgE leads to releasing of histamine and other mediators, which acts on specific receptors in small vessels, causing increasing permeability and dilatation and axon reflex stimulation • technique: prick/puncture or intradermal, small quantity of allergenic extract is introduced into the skin
4. assessment of allergy • SKIN TESTS • two control tests should be always performed: negative control - for exclusion of nonspecific reaction on pricking or solution used in production of extracts; positive control - for assessment of skin reactivity • size of skin weal recorded after 15 min. - measuring the mean diameter, positive test - a wheal at least 3 mm greater than negative control
Allergen SPECIFIC IgE • The advantages:- safety - high degree of precision - standardization - lack of dependence on the skin reactivity and medication • The disadvantages: - lack of immediately available results - high costs • Supplement to skin testing when the clinical significance of result is doubt • If immunotherapy is considered and lack of convincing history to confirm positive skin prick tests (concerns mites and moulds)
5. other tests • CHEST X - ray - • normal in asymptomatic asthma, necessary to exclude other diseases • acute asthma - hyperinflation and diagnosis of complication • BLOOD EOSINOPHIL COUNT - • increased count in about 50% of astma patients • predictive for responsiveness to therapy measure of the severity, indicates steroid requirement • SPUTUM EOSINOPHILIA • positive > 20% of the total leucocytes • usually present in symptomatic asthma
5. other tests • Exhaled nitric oxide (FeNO) • NO is produced in epithelial cells of the bronchial wall part of the inflammatory process • NO production increases with eosinophilic airway inflammation
Exhaled nitric oxide (FeNO) • Measure of airway inflammation • Derived from airway epithelial cells • Relatively easily measured (hand held device) –4 years and older • Reproducible, measurement takes secs
Conclusions • Asthma is a complex inflammatory disorder • Accurate detection of asthma remains difficult