Download
1 / 88
890 likes | 914 Views
Modeling the Cardiovascular and Respiratory Control Systems: Analysis and Applications. Seminar on Optimization and Control in Physiological Systems 2005. Jerry Batzel. General Outline. Respiratory physiology and a physiologically based model General modelin g considerations

E N D
Modeling the Cardiovascular and Respiratory Control Systems: Analysis and Applications Seminar on Optimization and Control in Physiological Systems 2005 Jerry Batzel
General Outline • Respiratory physiology and a physiologically based model • General modelin g considerations • Respiratory control system with delay • Stability analysis • Cardiovascular system model • Cardiovascular control system • Cardiovascular-respiratory system model • Optimal control considerations • Numerical implementation and Applications • Sleep transition • Congestive heart failure
Outline for First Part • Overview of respiratory physiology • Respiratory control system • Periodic breathing • A physiologically-based mathematical model • Variable cardiac output and state dependent delays • Sleep state • Applications • Congestive heart failure • Sleep apnea • Sudden Infant Death Syndrome (SIDS) • Existence and uniqueness of solution and stability analysis • Model validation against experimental data
General Considerations of Modeling I • Models should be only as complicated as needed for the problem under consideration • The design of a physiologically-based mathematical model needs to consider model validation: • Can model parameters be determined from data • Can the model explain known effects and predict new effects • Model Validation includes considering: • A priori identifiability: logical prerequisite. Does the model structure theoretically imply uniqueness of parameters determined from perfect data • Practical identifiability: Ís there sufficient accessible real data to determine the parameters of the system uniquely • Can new experiments provide extra data to determine parameters (issues of experimental design).
General Considerations of Modeling II • Parameter Identification involves methods of optimization to minimize deviations of model simulations from measured data as one varies the parameter set • With insufficient data, the estimated parameters may not be uniquely determined. That is, the calculated minimum may be a local minimum which the optimization scheme cannot escape from. This means that the estimated parameters may not be the physiologically true parameters that generated the data. • Model analysis includes considering: • The existence and uniqueness of solutions for the model system • The number of equilibrium points for the system • The conditions for stable and unstable behavior of the system
General Cardiovascular-Respiratory System • Six compartments: • Respiration:Lung,Tissue • Cardiovascular:pulmonary and systemic arterial and venous volumes • 13 state variables and one or more transport delays
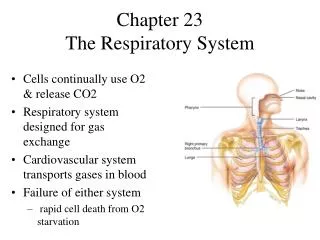
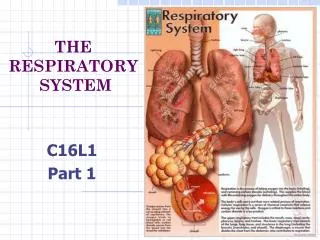
Respiratory Physiology • PURPOSE: Exchange CO2 for O2 • O2 is needed for metabolism in the body • CO2 is an unwanted gas byproduct of metabolism • The site of the gas exchange occurs at the boundary of the capillaries and the alveoli found in the lungs
Respiratory Physiology • 300 million (0.25-0.50 mm in diameter) alveoli • High surface area – 60 to 80 m2 • Gas exchange between the air and blood occurs entirely by diffusion through lung tissues • The primary determiner of diffusion is the partial pressure gradients • High surface area plus thin membranes separating the air and blood (2 cell width across) • Fast diffusion rate
Respiratory Control System • The control mechanism, which responds to the changing needs to acquire O2 and to expel CO2, acts to modulate both the blood flow and ventilation in a synchronized manner. • How the blood flow rate responds to the needs for O2 and how blood flow rate and ventilation rate are matched are not completely understood • The respiratory control mechanism is, however, much better understood
Respiratory Control System • Themost important factor in controlling ventilation is CO2 partial pressure of arterial blood • Regardless in daily levels of rest and activity, the CO2 partial pressure remains within 3mm Hg of the nominal level of 40mm Hg
Pons, medulla areas of brain Control Processor Sensors Effectors Chemoreceptors: central and peripheral Respiratory muscles Physiological Model of Ventilatory Control The control mechanism responds to the changing needs to acquire O2 and to expel CO2.
A Physiologically-Based Mathematical Model • Grodins, Buell and Bart (1966), Khoo et al. (1980’s and 1990’s) • Three compartments: • Lung • Tissue • Brain • Five state variables • Four transport delays
Lung compartment: Fick’s law • Tissue compartment: • Brain compartment: Metabolic rate Respiratory Compartment Equations
Fick’s law Inspired vs alveolar air Derivation of Lung Compartment Equation • Basic mass balance equations: • first term uses Fick’s Law • second term relates inspired vs alveolar air where .
Derivation of Lung Compartment Equation • Using Dalton’s law: and similarly where . Thus .
Derivation of Lung Compartment Equation • Using these relations: and substituting into we have .
Derivation of Lung Compartment Equation • Finally we relate concentration and partial pressure using the dissociation laws (in STPD): and . Substitution yields
Derivation of Lung Compartment Equation we also must relate STPD and BTPS units using the ideal gas laws resulting in the conversion factor: Substitution yields
Control function Respiratory Model Equations
Control Equation • The peripheral and central control, which effects on the ventilation rate, are additive • The central controller responds exclusively and linearly to arterial PCO2 as a steady state relation • The peripheral controller responds to both PCO2 and PO2 and is of the form
control gains Control Equation • A feedback control system of 5 differential equations • Coupled and nonlinear • Multiple delays • The airflow represents minute ventilation. • This model is due to Khoo et al. (1980’s and 1990’s), which is based on the seminal work by Grodins et al. (1966)
Tidal Volume and Ventilation • Dead space consists of the upper branches of airways and inspired air does not produce gas exchange in this region. Upon exhalation, air in this region has already equilibrated with pulmonary venous gases • Hence, at the beginning of the next inspiration the first fraction of air will not be as effective in gas exchange. • During exhalation there is also a reduced efficiency of gas exchange. • We model this with a reduction factor for minute ventilation during the inital phase of inspiration (dead space) and the exhilation phase.
10-20 sec. 10-20 sec. 10-20 sec. Periodic Breathing (PB) • The generic name given to a number of breathing patterns that are involuntary and have a regular pattern such as • Cheyne (1818) – Stokes (1854) Respiration (CSR) • Apneustic breathing • The understanding of PB has important medical applications because it occurs in • Patients with congestive heart failures • Sudden Infant Death Syndrome (SIDS) • Healthy mountain climbers (Mosso, 1898) and normal individuals during sleep
Negative Feedback What Causes PB? Decreased Ventilation Increased arterial PCO2 Plasma CO2 Blood pH Chemoreceptorsin medulla Chemoreceptorsin aortic and carotid bodies Time Delay Central Processorin medulla Spinal cord motor neurons Respiratory Muscles Increased Ventilation
Consider the control system Periodic Breathing Stability can be affected by time delays in the feedback loop • Well known in the control/dynamical system community where
Periodic Breathing • Infinite dimensional systems (Datko, 1989 and 1990) • Instability resulted from time delay in the feedback loop is also verified experimentally (Guyton et al., 1956) • Other factors (affecting stability): • High controller gain (will overcompensate for changes in the states, and thus, making the respiration control system to response in a highly volatile manner to small perturbation) • Sleep/arousal state (certain component, such as the lung, acts as a damping factor)
Parameters Congestive Heart Failure Nominal Central control gain Peripheral control gain Cardiac output Lung to brain delay Lung to tissue delay Lung to carotid artery delay Tissue to lung delay 1.8 mm Hg/min 0.14 mm Hg/min 6 l/min 12 sec 19 sec 10 sec 25 sec 1.88 mm Hg/min 0.135 mm Hg/min 3 l/min 21 sec 35 sec 17 sec 41 sec
Variable Blood Flow Rates • Blood flow to various regions of the bodydepends on a large number of factors: • Cardiac output, blood pressure, cross-section of arteries, and partial pressures of CO2 and O2 • Blood flow regulation (cardiovascular control system) is a very complicated phenomenon and is controlled by • Peripheral receptors similar to the respiratory control system which influence heart rate, heart contractility, and vascular resistance • Local mechanisms of resistance and compliance control • Cerebral blood flow is controlled locally in the brain by restricting or expanding the arterial vessels. • The degree of constriction depends on the partial pressure levels of CO2 and O2 and other local mechanisms
Brain Central Controller Both peripheral and brain arterial volume delays depend on cerebral blood flow Peripheral Controller Arterial volume delay depends on cardiac output To Tissue Compartment Heart State Dependent Delays • Transport delays depend onblood flow ratesto various areas • Using the models for cardiac output and cerebral blood flow, the transport delays are found by integrating the blood flow rates backward in time until the volumes are filled
The model equation reflecting these facts is: Normal Sleep Transition • Sleep condition involves different states with different physiological profiles. As one passes from stage 1 to stage 4 sleep: • CO2 response curve shifts rightward, response to overall ventilatory drive diminishes, and muscle resistance to the upper airways and other muscle groups related to breathing increases (loss of wakefulness stimuli) • Once stage 4 is reached the sleeper shifts NREM and REM (which affects the stability of the respiratory control system)
Sleep Apnea Apnea or cessation of breathing comes about in two ways: • Obstructive apnea (OA) which occurs when the upper airway collapses (loss of patency) blocking the flow of air to and from the lung • Central apnea or loss of ventilatory drive which can occur if the periodic swings in ventilatory drive reach zero (as seen in the congestive heart failure case due to the increased delay time in respiratory control)
Theoretical Considerations Assumptions: • PVCO2 is constant • PVO2 is constant • Cardiac output is constant • Only peripheral control is considered first Left with 2 equations describing arterial partial pressures of O2 and CO2
A Simplified Model • Two nonlinear delay differential equations with one constant delay
x -r t • The delay system has a unique positive equilibrium Existence and Uniqueness Results It can be shown that: • The delay system has a unique solution for every continuous initial data
Delay Dependent Stability Analysis • Linearizing the nonlinear delay system about the equilibrium solution, one can show (linear stability results):
Effects of Delay on Stability • Delay dependent stability is affected by • Controller gain • The manner in which changes in the ventilation rate is produced (i.e. deeper breathing is more unstable than faster breathing) • compartment volumes
, inspired air , and alveolar ventilation Dead space ventilation • Dead space ventilation is inspired air that does not produce gas exchange. • Dead space consists of the upper branches of airways and blocked or damaged alveoli (normally 25-30%). This effects Controller gain. If ventilation is changed by altering the depth of breathing: If ventilation is changed by altering the rate of breathing we have where
multiplying E F . • subtracting V D . in the control equation V A 3 D Model analytic results Dead space ventilation can be modeled by: or
3 D Model analytic results A E =0.7 F B . V =2.0 D