Download
1 / 15

E N D
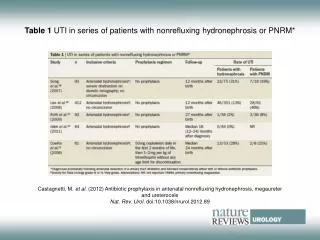
Hydronephrosis If the obstruction is in the urethra or bladder, hydronephrosis usually affects both kidneys; if the obstruction is in a ureter, it usually affects one kidney. Obstructions distal to the bladder cause the bladder to dilate and act as a buffer zone, delaying hydronephrosis. Total obstruction of urine flow with dilation of the collecting system ultimately causes complete atrophy of the cortex and cessation of glomerular filtration. Untreated hydronephrosis can result in infection, or pyelonephritis, due to stasis that exacerbates renal damage and may create a life-threatening crisis.
Wilms Tumour Is one of the most common primary neoplasms of young children. It usually presents between 3 and 5 years of age and is the most common malignant abdominal tumour in children. It may occur in one or both kidneys. Pathophysiology: Wilms tumour usually is a solitary mass that occurs in any part of the kidney. It usually is sharp demarcated and variably encapsulated. The tumours grow to a large size, distorting kidney structure. The tumours are staged using the National Wilms Tumour Study Group classification. Stage I: tumours are limited to the kidney and can be excised with the capsular surface intact. Stage II: tumours extend into the renal capsule but can be excised. Stage III: extension of the tumour is confined to the abdomen. Stage IV: haematogenous metastasis most commonly involves the lungs.
Wilms Tumour Porth, C.M. 2011. Essentials of Pathophysiology, 3rd edn.
Assessing Your Understanding Most kidney stones are _______________ stones. An acute episode of ___________________ is characterised by frequent urination, lower abdominal or back discomfort, and burning and pain on urination. Acute post-infectious glomerulonephritis usually occurs after infection with certain strains of group A B- haemolytic streptococci and is caused by _______________ of immune complexes. _____________ is one of the most common primary neoplasms of young children.
Acute Renal Failure Acute renal failure is the sudden interruption of renal function. It can be caused by obstruction, poor circulation, or kidney disease. It is potentially reversible, however, if left untreated, permanent damage can lead to chronic renal failure. Pathophysiology: Acute renal failure may be classified as pre-renal, intra-renal, or post-renal. Each type has different causes: Pre-renal failure: results from conditions that diminish blood flow to the kidneys. Examples include hypovolemia, hypotension, vasoconstriction or inadequate cardiac output. Intrarenal failure, also called intrinsic or parenchymal renal failure, results from damage to the filtering structures of the kidneys, usually from acute tubular necrosis, a disorder that causes cell death or from nephrotoxic substances such as certain antibiotics. Post-renal failure results from bilateral obstruction of urine outflow, as in prostatic hyperplasia or bladder outlet obstruction.
Causes of Acute Renal Failure Hendler, C.B. 2002. Pathophysiology made ridiculously easy, 2nd edn.
Acute Renal Failure: How it Happens Robinson, J.M. 2005. Pathophysiology: Just the facts.
Chronic Renal Failure Chronic renal failure, usually progressive and irreversible deterioration, is the end result of gradual tissue destruction and loss of kidney function. Occasionally, however, chronic renal failure results from a rapidly progressing disease of sudden onset that destroys the nephrons and causes irreversible kidney damage. Pathophysiology: Chronic renal failure typically progresses through four stages, it may result from: Chronic glomerular disease, such as glomerulonephritis, which affects the capillaries in the glomeruli. Congenital anomalies such as polycystic kidney disease. Vascular diseases, such as hypertension and nephrosclerosis, which causes hardening of the kidneys. Obstruction such as renal calculi Collagen diseases such as lupus erythematous Nephrotoxic agents such as long-term aminoglycoside therapy Endocrine diseases such as diabetic neuropathy
Chronic Renal Failure Nephron damage is progressive. Once damaged, nephrons are no longer able to function. Healthy nephrons compensate for destroyed nephrons by enlarging and increasing their clearance capacity. The kidneys can maintain relatively normal function until about 75 percent of the nephrons are non-functional. Eventually, the healthy glomeruli are so overburdened they become sclerotic and stiff, leading to their destruction as well. If this condition continues unchecked, toxins accumulate and produce potentially fatal changes in all major organ systems. Even if a patient can tolerate life-sustaining maintenance dialysis or a kidney transplant, he/she may still have anaemia, nervous system effects, cardiopulmonary and GI complications, sexual dysfunction and skeletal defects.
Chronic Renal Failure: How it Happens Robinson, J.M. 2005. Pathophysiology: Just the facts.
Pathophysiologic Changes Fluid and electrolyte imbalances Loss of bicarbonate Accumulation of toxins Altered metabolic processes Endocrine disturbances: infertility, decreased libido, amenorrhoea, impotence. Thrombocytopenia and platelet defects Decreased macrophage activity
Marking Guidelines Adherence to all requirements: Did you select 4 of the listed conditions?; Did you answer every question?; Did you adhere to word count?; Did you use relevant and current sources of information to substantiate your claims. Accuracy of content: Are your statements substantiated by reliable and valid scholarly literature. Is the content reflective of current medical management? Currency of Information: Use of reputable sources of information; Use of a range of sources i.e. journal articles. Action Plan and its implementation: Key headings outlining your action plan and an explanation (one paragraph) of how each heading corresponds to the pathogenic course of the condition; Implementation (i.e. time frame); Public education campaigns. Record Keeping Discussion: What questions do you need to ask a potential client presenting with this condition? The most practical way of putting this together is in table form, with a checklist.