Download
1 / 64
720 likes | 1.59k Views
May 2016. Hydronephrosis. Hydronephrosis. Hydronephrosis & hydroureter : Common clinical conditions encountered not only by urologists but also by emergency medicine specialists and primary care physicians

E N D
May 2016 Hydronephrosis
Hydronephrosis • Hydronephrosis& hydroureter: Common clinical conditions encountered not only by urologists but also by emergency medicine specialists and primary care physicians • Hydronephrosis defined: Distention of renal calyces & pelvis with urine as a result of obstruction of outflow of urine distal to renal pelvis • Hydroureter defined: Dilation of ureter Lusaya DG, et al. Medscape. 2015.
Hydronephrosis Normal kidney
Hydronephrosis • Presence of hydronephrosis or hydroureter can be physiologic or pathologic • May be acute or chronic, unilateral or bilateral • Can be secondary to obstruction of urinary tract, but it can also be present even without obstruction Lusaya DG, et al. Medscape. 2015.
Hydronephrosis • Obstructive uropathy: Functional or anatomic obstruction of urinary flow at any level of urinary tract • Obstructive nephropathy: Obstruction causes functional or anatomic renal damage • Thus, the terms hydronephrosis & obstruction should not be used interchangeably Lusaya DG, et al. Medscape. 2015.
Etiology • Etiology & presentation of hydronephrosisand/or hydroureterin adults differ from that in neonates & children • Anatomic abnormalities (including urethral valves or stricture & stenosis at ureterovesicalor ureteropelvicjunction) account for majority of cases in children • Calculi are most common in young adults • Prostatic hypertrophy or carcinoma, retroperitoneal or pelvic neoplasms & calculi are primary causes in older patients Lusaya DG, et al. Medscape. 2015.
Hydronephrosis in pregnancy • Hydronephrosis or hydroureter: Normal finding in pregnant women • Renal pelvises & calicealsystems may be dilated as a result of progesterone effects & mechanical compression of ureters at pelvic brim • Dilatation of ureters & renal pelvis is more prominent on right side than left side and is seen in up to 80% of pregnant women • These changes can be visualized on ultrasound examination by 2nd trimester & they may not resolve until 6-12 weeks post partum Lusaya DG, et al. Medscape. 2015.
Pathophysiology • Hydronephrosis can result from anatomic or functional processes interrupting flow of urine • This interruption can occur anywhere along urinary tract from kidneys to urethral meatus • Rise in ureteral pressure leads to marked changes in glomerular filtration, tubular function & renal blood flow • Glomerular filtration rate (GFR) declines significantly within hours following acute obstruction. This significant decline of GFR can persist for weeks after relief of obstruction Lusaya DG, et al. Medscape. 2015.
Pathophysiology • Renal tubular ability to transport sodium, potassium & protons and concentrate and to dilute the urine is severely impaired • Extent & persistence of these functional insults is directly related to duration and extent of obstruction • Brief disruptions are limited to reversible functional disturbance with little associated anatomic changes • More chronic disruptions lead to profound tubular atrophy and permanent nephron loss Lusaya DG, et al. Medscape. 2015.
Pathophysiology • Increased ureteral pressure also results in pyelovenous& pyelolymphatic backflow • Gross changes within urinary tract similarly depend on duration, degree & level of obstruction • Within intrarenal collecting system, degree of dilation is limited by surrounding renal parenchyma • However, extra-renal components can dilate to point of tortuosity Lusaya DG, et al. Medscape. 2015.
Acute and chronic hydronephrosis • Acute as hydronephrosis: When corrected, allows full recovery of renal function • Chronic hydronephrosis: Loss of function is irreversible even with correction of obstruction • Animal experiments: If acute unilateral obstruction is corrected within 2 weeks, full recovery of renal function is possible. However, after 6 weeks of obstruction, function is irreversibly lost Lusaya DG, et al. Medscape. 2015.
Acute and chronic hydronephrosis • Grossly, acutely hydronephrotic system can be associated with little anatomic disturbance to renal parenchyma • Chronically dilated system may be associated with compression of papillae, thinning of parenchyma around calyces & coalescence of septa between calyces • Cortical atrophy progresses to point at which only a thin rim of parenchyma is present Lusaya DG, et al. Medscape. 2015.
Acute and chronic hydronephrosis • Microscopic changes consist of dilation of tubular lumen & flattening of tubular epithelium • Fibrotic changes & increased collagen deposition are observed in peritubular interstitium Lusaya DG, et al. Medscape. 2015.
Causes • A multitude of causes exist for hydronephrosis& hydroureter • Classification can be made according to level within urinary tract & whether etiology is intrinsic, extrinsic or functional Lusaya DG, et al. Medscape. 2015.
Intrinsic ureter level • Causes can be as follows: • Ureteropelvic junction stricture • Ureterovesical junction obstruction • Papillary necrosis • Ureteral folds • Ureteral valves • Ureterovesical reflux • Ureteral stricture (iatrogenic) • Blood clot Lusaya DG, et al. Medscape. 2015.
Intrinsic ureter level • Causes can be as follows: • Benign fibroepithelial polyps • Ureteral tumor • Fungus ball • Ureteral calculus • Ureterocele • Endometriosis • Tuberculosis • Retrocaval ureter Lusaya DG, et al. Medscape. 2015.
Functional ureter level • Causes can be as follows: • Gram-negative infection • Neurogenic bladder Lusaya DG, et al. Medscape. 2015.
Extrinsic ureter level • Causes can be as follows: • Retroperitoneal lymphoma • Retroperitoneal sarcoma • Cervical cancer • Prostate cancer • Retroperitoneal fibrosis • Aortic aneurysm • Inflammatory bowel disease • Ovarian vein syndrome • Retrocaval ureter • Uterine prolapse Lusaya DG, et al. Medscape. 2015.
Extrinsic ureter level • Causes can be as follows: • Pregnancy • Iatrogenic ureteral ligation • Ovarian cysts • Diverticulitis • Tuboovarian abscess • Retroperitoneal hemorrhage • Lymphocele • Pelvic lipomatosis • Radiation therapy • Urinoma Lusaya DG, et al. Medscape. 2015.
Bladder • Intrinsic bladder level causes can be as follows: • Bladder carcinoma • Bladder calculi • Bladder neck contracture • Cystocele • Primary bladder neck hypertrophy • Bladder diverticula • Functional bladder level causes can be as follows: • Neurogenic bladder • Vesicoureteral reflux • Extrinsic bladder level causes can include pelvic lipomatosis Lusaya DG, et al. Medscape. 2015.
Urethra • Intrinsic urethra level causes can be as follows: • Urethral stricture • Urethral valves • Urethral diverticula • Urethral atresia • Labial fusion • Hypospadias & epispadias • Extrinsic urethra level causes can be as follows: • Benign prostatic hyperplasia • Prostate cancer • Urethral & penile cancer • Phimosis Lusaya DG, et al. Medscape. 2015.
Urinary Tract Obstruction • Obstructions in urinary tract: Reduce urinary flow: Impair renal function • Frequent effect of partial or complete obstruction is dilation of renal pelvic (hydronephrosis) • Obstructions of urinary tract are painful & need immediate treatment
Congenital pelviureteric junction obstruction Calculi • Cancer of • Ovary • Cervix • Uterus Retroperitoneal fibrosis, tumours, haemorrhage Functional: vesicoureteric reflux Neurogenic bladder Bladder cancer Prostatic hypertrophy or cancer Types & locations
Clinical features • Symptoms vary depending on whether hydronephrosisis acute or chronic • With acute obstruction, pain is frequently present, due to distention of bladder, collecting system, or renal capsule • Pain is typically minimal or absent with partial or slowly developing obstruction (as with congenital ureteropelvic junction [UPJ] obstruction or a pelvic tumor). It is not uncommon, for example, to see an adult who is noted to have hydronephrosis due to previously unsuspected UPJ obstruction Lusaya DG, et al. Medscape. 2015.
Clinical features • Relatively severe pain (renal or ureteral colic) may be seen with acute complete obstruction (as with a ureteral calculus) or when acute dilatation occurs after a fluid load that increases urine output to level greater than flow rate through area of obstruction • An example of latter problem occurs after beer drinking in a college student with previously asymptomatic & unsuspected UPJ obstruction • Site of obstruction determines location of pain: Upper ureteral or renal pelvic lesions lead to flank pain or tenderness, whereas lower ureteral obstruction causes pain that may radiate to ipsilateral testicle or labia Lusaya DG, et al. Medscape. 2015.
Clinical features • With regard to renal insufficiency, patients with complete or severe partial bilateral obstruction also may develop acute or chronic renal failure. In the latter setting, patient is often asymptomatic & urinalysis results may be relatively normal or reveal only few white or red blood cells • Anuria may be a presenting symptom of patient. Although urine volume could be reduced in any form of renal disease, anuria is most often seen in 2 conditions: complete bilateral urinary tract obstruction & shock Lusaya DG, et al. Medscape. 2015.
Clinical features • Other less common causes of anuria: • Hemolyticuremic syndrome • Renal cortical necrosis • Bilateral renal arterial obstruction & crescentic or rapidly progressive glomerulonephritis, particularly anti–glomerular basement membrane (GBM) antibody disease Lusaya DG, et al. Medscape. 2015.
Clinical features • A history of hematuria may herald a stone or malignancy anywhere in urinary tract • A history of fever or diabetes adds urgency to evaluation & treatment • A history of a solitary kidney is an emergent situation • Hydronephrosis may develop silently, without symptoms, as result of advanced pelvic malignancy or severe urinary retention from bladder outlet obstruction • Bilateral symmetrical hydronephrosis usually suggests a cause related to bladder, such as retention, prostatic blockage, or severe bladder prolapse Lusaya DG, et al. Medscape. 2015.
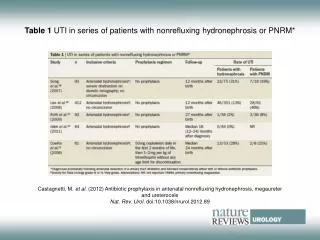
Pediatric hydronephrosis and hydroureter • Fetalhydronephrosis is readily diagnosed finding on antenatal ultrasound examination & can be detected as early as 12th - 14th week of gestation • Although renal pelvic dilatation is transient, physiologic state in most cases, urinary tract obstruction & vesicoureteral reflux (VUR) are also causal • Most cases of antenatal hydronephrosis are not clinically significant & can lead to unnecessary testing of newborn baby and anxiety for patients and healthcare providers Lusaya DG, et al. Medscape. 2015.
Physical • With severe hydronephrosis, kidney may be palpable • With bilateral hydronephrosis, lower extremity edema may occur • Costovertebral angle tenderness on affected side is common • A palpably distended bladder adds evidence of lower urinary tract obstruction • A digital rectal examination should be performed to assess sphincter tone & to look for hypertrophy, nodules, or induration of prostate Lusaya DG, et al. Medscape. 2015.
In children • Physical examination, especially in a newborn, can help detect abnormalities that suggest genitourinary abnormalities associated with antenatal hydronephrosis. These include the following: • Presence of abdominal mass could represent an enlarged kidney due to obstructive uropathy or multicystic dysplastic kidney (MCDK) • A palpable bladder in male infant, especially after voiding, may suggest posterior urethral valves • A male infant with prune belly syndrome will have deficient abdominal wall musculature & undescended testes • Presence of associated anomalies should be noted Lusaya DG, et al. Medscape. 2015.
In children • Presence of outer ear abnormalities is associated with increased risk of congenital anomalies of kidney & urinary tract (CAKUT) • A single umbilical artery is associated with increased risk of CAKUT, particularly VUR Lusaya DG, et al. Medscape. 2015.
Investigations • Straight abdomen of X- ray • Excretory urography • Retrograde urography • Ultrasound
Medical care • Role of medical treatment of hydronephrosis& hydroureterin adults is limited to pain control & treatment or prevention of infection • Most conditions require either minimally invasive or open surgical treatment • 2 notable exceptions are (1) oral alkalinization therapy for uric acid stones & (2) steroid therapy for retroperitoneal fibrosis Lusaya DG, et al. Medscape. 2015.
Medical care • Management approach to infants with antenatal hydronephrosis is based on confirmation of persistent postnatal hydronephrosis& following 2 predictive factors: • Bilateral involvement • Severe hydronephrosis: Fetuses with renal pelvic diameter < 15 mm during 3rd trimester are at greatest risk for significant renal disease Lusaya DG, et al. Medscape. 2015.
Bilateral hydronephrosis • Infants with severe bilateral antenatal hydronephrosis and/or bladder distension are at increased likelihood of having significant disease • These infants and those with severe hydronephrotic solitary kidney should be evaluated initially by ultrasonography on 1st postnatal day • Bilateral hydronephrosis suggests obstructive process at level of or distal to bladder, such as ureteroceleor posterior urethral valves (PUV) in male infant, which can be associated with impaired renal function & ongoing renal injury Lusaya DG, et al. Medscape. 2015.
Bilateral hydronephrosis • If postnatal ultrasonography demonstrates persistent hydronephrosis, voiding cystourethrography(VCUG) should be performed • In male infants: Posterior urethra should be fully evaluated to detect possible PUVs • Infants with mild or moderate hydronephrosis can be evaluated after 7 days of life Lusaya DG, et al. Medscape. 2015.
Severe unilateral hydronephrosis • In newborns with severe antenatal unilateral hydronephrosis (renal pelvic diameter >15 mm in 3rd trimester), ultrasonography should be performed after infant returns to birth weight (after age 48 h & within 1st 2 wk of life) Lusaya DG, et al. Medscape. 2015.
Moderate & mild unilateral hydronephrosis • In newborns with less severe antenatal unilateral hydronephrosis (renal pelvic diameter < 15 mm during 3rd trimester), ultrasonography can be performed after age 7 days to see whether hydronephrosis has persisted postnatally Lusaya DG, et al. Medscape. 2015.
Moderate & mild unilateral hydronephrosis • Moderate hydronephrosis resolves by age 18 months in most cases. This was illustrated by prospective study of 282 infants (age 2 mo) with renal pelvic diameters between 10 & 15 mm, which resolved in 94% of patients by age 12-14 months (resolution was defined as renal pelvic diameter ≤5 mm on 2 consecutive ultrasounds) • Of 18 patients with persistent hydronephrosis, 14 had ureteropelvic junction (UPJ) obstruction & 4 had vesicoureteral reflux (VUR) Lusaya DG, et al. Medscape. 2015.
Treatment • Secondary hydronephrosis: Treatment of cause • Primary hydronephrosis: • Pyeloplasty: • Anderson- Hynes • Culp • Foley • Nephrectomy
Anderson-Hynes pyeloplasty Khan F, et al. Nature Reviews Urology 11, 629–638 (2014).