Download
1 / 30
310 likes | 560 Views
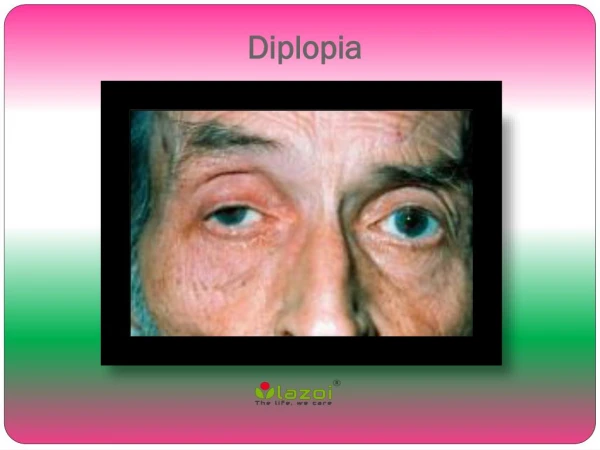
Diplopia post sinus surgery. Orly H alachmi , Lionel Kowal Alumni 17-10-11 RVEEH. C.L. 79 y o lady c/o: P ost sinus surgery diplopia (worse in RG, lately affecting PP), shuts one eye when reading. POHx : Bilateral PKE P/C + Yag Capsulotomy . Press-on prism – did not help. C.L.

E N D
Diplopia post sinus surgery Orly Halachmi, Lionel Kowal Alumni 17-10-11 RVEEH
C.L. • 79 y o lady • c/o: Post sinus surgery diplopia (worse in RG, lately affecting PP), shuts one eye when reading. • POHx: Bilateral PKE P/C +YagCapsulotomy. • Press-on prism – did not help.
C.L • O/E: • VA : R 6/12 L 6/7cc • N4 R+L Titmus200’’ • AT 12/16 • L Fundus Extortion
CL in P.P CT: X <--> LXT N X’=25 ^ D X(T) = 18 ^ RHypoT=4 Changes : Dip <–> fusion
RG XT LMR- R HypoT
OM: R UG LIO+
Abnormal morphology of the LSO and LMR compared with normal Rt side.
No intervening fat between LMR and orbital wall, nor between L SO and MR (compared to the Rt).
Plan Options: 1. To try to free up the muscle from where it is stuck to the bone (has an appointment with orbital doctor). 2. Do a Muscle Sxw/o correcting the orbital wall/ freeing the Muscles.
Option 2 a. Surgery • LIO weakening procedure. • LMR resection • If LLR tight LLR recession. * Since this will make her ET in LG , she needs yoke muscle RMR recession (adjustable). b. BOTOX to the LLR/LIO (less reliable results than Sx).
C Rene, G E Rose, R Lenthall, I Moseley. Major orbital complications of endoscopic sinus surgery. Br J Ophthalmol2001;85:598–603) Literature 1 • A retrospective review of four cases of severe orbital trauma during endoscopic sinus surgery. • Allthe cases suffered MR damage, • Onehad additional injury to the IR and IO, and • Two patients were blinded due to direct damage to the optic nerve or its blood supply. ---------------------------------------------------------------
MR injury • The MR is adjacent to the lamina papyraceaand was injured in all (4/4) pt’s due to direct loss of muscle/entrapment. • The injury is associated with divergent strabismus, with almost absent of aDduction. • Also likely a damage to the nerve/vascular supply to the muscle - in which case a slow recovery of aDductionis anticipated.
ON injury • 2/4 pt’s suffered blindness due to direct optic nerve damage. • The intraorbital ON can be damaged by instruments entering the orbit/ by distraction of tissues from the orbit into the ethmoidectomy site.
Predisposed factors for inadvertent orbital entry during ethmoid sinus Sx. • Nasal approach (rather than extraorbital); • A very thin/incomplete lamina papyracea; • Anatomical variants in the sinus/when using sinus debridement; • Disruption of normal anatomy from disease or previous Sx.
Awareness that this can be a complication hence, • Assess pre-op with a CT scan: info about the extent of the sinus disease, anatomical variants and lamina papyracea location. • Periodically uncover the eyes during Sx. Monitor: sudden swelling/ bruising, proptosis, eyeball movements (d/t traction on orbital fat), dilated/ poorly reactive pupiland RAPD, tense proptotic orbit and compressive optic neuropathy d/t orbital hemorrhage.
Ophthalmic treatment • A Hx of Dip post sinus surgery and a motility defect is strongly suggestive of orbital entry during sx. • If enophthalmos or muscle entrapment plan orbital exploration and release of entrapped tissues strabismus surgery. • If no MR entrapment consider inducing paralysis of the Ipsi lateral antagonist with BTX to minimize contracture while awaiting recovery of the orbital soft tissue injury. Later, repair of the large angle XT or X(T). • Should the MR be essentially absent, then medial transposition of the vertical recti may be required with botulinum toxin paralysis of the LR.
Literature 2 • 30 cases from 1994 to 2000 gathered from 10 centers. • 16 men and 14 women. • Mean age: 45 years (range, 20 - 76 years). • Follow-up from initial injury: 12m (2- 48m). • A spectrum of MR injury: simple contusion to complete MR transection, w and w/o entrapment. Christine M. Huang, et al. Medial Rectus Muscle Injuries Associated With Functional Endoscopic Sinus Surgery (Ophthalmic Plastic and Reconstructive Surgery), 2002
Four general patterns of presentation and corresponding injuries were categorized: • Our pt is pattern II • Tx in group I and II (MR tissue loss), were challenging. • Observation / IV steroids alone did not result in improved ocular alignment. • Early exploration of the entrapped muscle with suturing the muscle remnants, BTX injection to the ipsilateralantagonist (LR), improved primary ocular alignment. • Late orbital exploration had limited results. • Vertical rectus muscle transposition as a secondary late procedure variable improvement on ocular motility.
Discussion(1) • The incidence of ocular complications during sinus Sxis low, but when they occur- have significant morbidity. • With increasing interest in endoscopic sinus surgery, more ocular complications are likely to occur. • MR, the most commonly injured extraocular muscle (direct laceration, neurovascular interruption, entrapment or adhesions to adjacent structures). • Post-op CT is important in assessing the medial wall, the MR and surrounding orbital soft tissues and the size and location of the medial wall bony defect.
Discussion (2) Treatment of the MR injury includes: • Early exploration (within 2- 3/52), freeing or repair of entrapped tissues, and cover the bony defect with an implant if necessary. • Reattachment of the lacerated ends of the MR improves PP alignment. • Adjunctive weakening of the antagonist LR with BTX injection (5 units under direct visualization). • Vertical transposition if MR transected, to improve aDduction.