Download
1 / 21
210 likes | 220 Views
Con Position: APRV should be used in ARDS. Timothy Scialla, MD Assistant Professor Division of Pulmonary and Critical Care Duke University 09/07/2017. COI disclosure slide. I am a co-investigator for on-site clinical research trials sponsored by: GSK AstraZeneca Sanofi Genentech NHLBI.

E N D
Con Position: APRV should be used in ARDS Timothy Scialla, MD Assistant Professor Division of Pulmonary and Critical Care Duke University 09/07/2017
COI disclosure slide • I am a co-investigator for on-site clinical research trials sponsored by: • GSK • AstraZeneca • Sanofi • Genentech • NHLBI
ARDS epidemiology • 190,000 cases / year in the USA • 50% Moderate (PaO2/FiO2 100-200) • 25% Severe (PaO2/FiO2 < 100) • Mortality 40% • Early (underlying cause) • Late (sepsis / nosocomial pneumonia /MODS) • Ventilatory failure (ie. Hypoxemia) uncommon • High Morbidity (cognitive, psychological, physical)
The ARDS Industrial Complex • Nearly 2 decades of well-funded research • Multiple large randomized trials • Pharmacotherapy • Ventilator strategies • Hemodynamic monitoring/management • Lessons learned • Heterogeneous disease process • Different ARDS phenotypes • Few successes Extensive Animal Studies
Studies with mortality benefit • ARMA trial • Neuromuscular blockade in ARDS • Prone positioning in ARDS • All three: • Avoid ventilator-induced lung injury
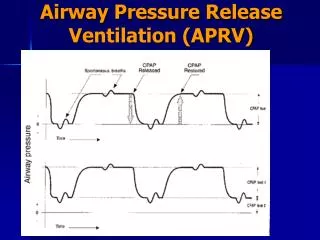
The ventilator is an agent of harm Risk of overdistension injury 12 12 Lung volume 6 6 6 6 Risk of atelectasis injury Time
Lung Protective Strategies • “Low VT” strategy • Minimize stress and strain • Limit VT and plateau pressure (<30cm H20) • “Open Lung” strategy: • recruiting nonaerated lung regions • Keep open with adequate levels of PEEP. • Minimize hyperinflation and atelectrauma with alveolar recruitment.
ARDS Network Low vs. Traditional VT P=0.007 6 ml/kg 12 ml/kg • Absolute risk reduction = 9% (31% vs 40% mort) • Relative risk reduction = 22% Lower oxygenation Worse ventilation ARDS Network NEJM 2000
Lung Protective Ventilation and Knowledge Translation Needham et al. BMJ. 2012 • 180/485 patients (37%) never had LPV • 417/485 (86%) adherent 50% or less
NMB in early ARDS. Papazian et. al. NEJM. 2010 • 340 patients randomized • Sedative: Ramsey Level = 6 (very very sedated) • Cisatracurium group: • 15mg bolus followed by continuous infusion for 48hrs • Open label 20mg IV bolus of cisatracurium allowed in either group if Pplat>32. Adjusted Cox regression model: HR 0.68 (95% CI, 0.48 to 0.98; p=.04) Adjustments made for PaO2/FiO2; Pplat, SAPS II
Open Lung Strategy:Metaanalysis: High vs Low PEEP. • Higher PEEP (n=1136) Low PEEP (n=1163) • Higher PEEP: better PaO2 transiently (same at day 7) • Higher PEEP: Pplat; PEEP Briel et al. JAMA. 2010
Why these results? Responders Nonresponders Grasso et al. High vs Low PEEP. AJRCCM. 2005.
HFO: The perfect scenario Risk of overdistension injury Lung volume Risk of atelectasis injury Time
Avoid this Risk of overdistension injury Lung volume Risk of atelectasis injury Time
HFOV: Our curiosity with this mode has come to an end • OSCILLATE trial • 548 patients • HFO group • Increased sedation/paralytics • More pressors/high mean airway pressures • Less refractory hypoxemia • Increased mortality? N=146 P=.08 Ferguson et al. NEJM. 2013
Prone Positioning in ARDS: Mount Everest in Kansas • Recruited more severely hypoxemic patients • Prone group with higher PaO2:FiO2 ratio at days 3 and 5 • Prone group had lower Pplatrs lower at days 3 and 5 • NNT to prevent one death was 6 Guerin et al. NEJM. 2013
Pleural pressure in dependent and non-dependent regions Fessler and Talmor. Respiratory Care. 2010
APRV: Evidence & Limitations • Evidence • Limited, small, mostly trauma patients • One RCT: APRV vs LOVT • Intubated trauma patients at risk for ARDS • LOVT = SIMV (VT = 6ml/kg PS=10 cm H20) • Limitations • At Phigh: spont breaths can add to strech • Plow to Phigh: shearing/atelectrauma N=31 N=32 Maxwell et al. J Trauma. 2010
Conclusions • 2 decades of extensive prospective studies • APRV = 1 very small RCT (negative study) • Longer time on ventilator • No improvements in oxygenation • Trend towards more sedation! • Low tidal volume ventilation is GOLD STANDARD • Severe cases • Neuromuscular blockage • Prone ventilation • Neither requires tertiary care center/ high technology