Download
1 / 32
320 likes | 446 Views
Health and Social Care Bill 2011. Local Democratic Legitimacy in health. The review of arms length bodies. Regulating Healthcare providers. Transparency in outcomes: a framework for the NHS. Commissioning for Patients.

E N D
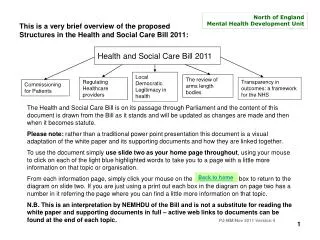
Health and Social Care Bill 2011 Local Democratic Legitimacy in health The review of arms length bodies Regulating Healthcare providers Transparency in outcomes: a framework for the NHS Commissioning for Patients The Health and Social Care Bill is on its passage through Parliament and at present is on pause whilst a listening exercise is carried out. The content of this document is drawn from the Bill as it stands and will be updated after publication of the outcomes of the listening exercise. Please note: rather than a traditional power point presentation this document is a visual adaptation of the white paper and its supporting documents and how they are linked together. To use the document simply use slide two as your home page throughout, using your mouse to click on each of the light blue highlighted words to take you to a page with a little more information on that topic or organisation. From each information page, simply click your mouse on the box to return to the diagram on slide two. If you are just using a print out each box in the diagram on page two has a number in it referring the page where you can find a little more information on that topic. N.B. This is an interpretation by NEMHDU of the Bill and is not a substitute for reading the white paper and supporting documents in full – active web links to documents can be found at the end of each topic. PJ-MM/May 2011 Version 2 final This is a very brief overview of the proposed structures in the Health and Social Care Bill 2011: Back to home 1
Secretary of state NHS Outcomes Framework 3 Public Health Outcomes framework 5 Adult Social Care Outcomes Framework 7 Overlapping frameworks diagram can be found on page 8 NHS Commissioning board 10 NICE 11 Public Health England 12 CQC 13 Health Watch England 14 Monitor 15 Office of Fair Trading17 Commissioning outcomes framework 19 Local Health Watch 25 Public Health 24 National and Regional Specialist Commissioning 20 G.P Consortia 21 Health & Wellbeing Boards 28 Local Authority 23 Foundation Trusts 30 Family Health services J.S.N.A. 29 Timeline of changes can be found on page 9 GP Practices 32 Primary Medical Care Joint Health and Wellbeing Strategy 29 Maternity Services Not Midwives Independent sector Health in Criminal Justice system 2 Patients carers and the public
The NHS Outcomes Framework 2011/12 This first NHS Outcomes Framework sets out the outcomes and corresponding indicators that will be used to hold the NHS Commissioning Board to account for the outcomes it secures through its oversight of the commissioning of health services from 2012/13. The indicators used to hold NHS organisations to account during 2011/12 were set out in The Operating Framework for the NHS in England in 2011/12 which provided the financial, business and planning rules that support the delivery of NHS priorities. • For 2011/12, levels of ambition have not been attached to the indicators and the NHS will not be held to account for progress against these. Rather, the framework is intended to set the direction of travel, with the transition year ahead offering an opportunity for the NHS to begin to think through what an NHS focused on outcomes will mean for individuals, organisations and whole health economies. • During 2011/12, we will work to refine the indicators in the framework and finalise precise definitions where necessary. Where data is available, 2011/12 will be used to identify baselines. This year will also be used to negotiate levels of ambition with the shadow NHS Commissioning Board, in light of the NHS settlement following the 2010 Spending Review. • In 2012/13, the framework will be used by the Secretary of State for Health to hold the NHS Commissioning Board to account and for achieving levels of ambition where they have been agreed. Continued on next page
NHS Outcomes Framework continued... The NHS outcomes framework is made up of five domains and the following diagram illustrates how each domain influences the NHS quality improvement system Back to home Domain 1 Preventing people from dying prematurely Domain 2 Enhancing quality of life for people with long term conditions Domain 3 Helping people to recover from episodes of ill health or following injury Domain 4 Ensuring that people have a positive experience of care Domain 5 Treating and caring for people in a safe environment and protecting them from avoidable harm NICE Quality Standards (Building a library of approx 150 over 5 years) Provider payment mechanisms Commissioning Outcomes Framework Commissioning Guidance tariff Standard contract CQUIN QOF Commissioning/Contracting NHS Commissioning Board – certain specialist services and primary care GP Consortia – all other healthcare services NHS Outcomes Framework information taken from: The NHS Outcomes Framework 2011/12 http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_123138.pdf 4
Proposals for a Public Health Outcomes Framework The forthcoming Outcomes Framework will have to reflect the collective responsibility of communities, local authorities and their partners and the role of Government in improving and protecting health. To do this, we have been guided by the following principles to develop the Outcomes Framework. It will: • use indicators which are meaningful to people and communities; • focus on major causes and impacts of health inequality, disease, and premature mortality; • take account of our legal duties in particular under equalities legislation and regulations. • take a life course approach, and • as far as possible, use data collated and analysed nationally to reduce the burden on local authorities. The outcomes framework will have three main purposes: • To set out the Governments goals for improving and protecting the nation’s health, and for narrowing health inequalities through improving the health of the poorest fastest; • To provide a mechanism for transparency and accountability across the public health system at the national and local level for health improvement and protection and inequalities reduction; and • To provide the mechanism to incentivise local health improvement and inequalities reduction against specific public health outcomes through the “health premium” Continued on next page
Back to home Proposals for a Public Health Outcomes Framework continued… The purpose is to put in place a new strategic outcomes framework for public health at national and local levels based on the evidence of where the biggest challenges are for health and wellbeing and is based on five domains: • Domain 1: Health Protection and Resilience: protect the population from major emergencies and remain resilient to harm • Domain 2: Tackling wider determinants of health: tackling factors which affect health and wellbeing and health inequalities. • Domain 3: Health Improvement: Helping people to live healthy lifestyles, make healthy choices and reduce health inequalities. • Domain 4: Prevention of Ill health: reducing the number of people living with preventable ill health and reduce health inequalities. • Domain 5: Healthy Life expectancy and preventable mortality: preventing people from dying prematurely and reduce health inequalities. Information taken from: Healthy Lives, Healthy People: Transparency in Outcomes. Proposals for a Public Health Outcomes Framework. http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_123113.pdf
Back to home Transparency in outcomes: a framework for adult social care The adult social care outcomes framework sets out agreed outcome measures in four domains: • Enhancing quality of life for people with care and support needs • Delaying and reducing the need for care and support • Ensuring that people have a positive experience of care and support • Safeguarding adults whose circumstances make them vulnerable and protecting from avoidable harm • These outcomes, combined with other resources such as the Adult Social Care Survey, will inform the ‘local account’, which is a new way for councils and local communities to have a more detailed and meaningful dialogue. The local account will replace previous annual publications by the Care Quality Commission. View overlapping outcome frameworks diagram Information taken from: Transparency in outcomes; a framework for quality in adult social care http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_125686.pdf
The three overlapping frameworks for the NHS, public health and adult social care services Public Health Adult Social Care and Public Health Maintaining good health and wellbeing. Preventing avoidable ill health or injury, including through reablement or intermediate care services and early intervention. NHS and Public Health Preventing ill health and lifestyle diseases and tackling their determinants. Adult Social Care and NHS Supported discharge from NHS to social care. Impact of reablement or intermediate care services on reducing repeat emergency admissions. Supporting carers and involving in care planning. Adult Social Care NHS Adult Social Care, NHS and Public Health The focus of Joint Strategic Needs Assessment: shared local health and wellbeing issues for joint approaches. Continue to timeline Information taken from: Healthy Lives, Healthy People: Transparency in outcomes; proposals for a public health outcomes framework – a consultation document http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_123113.pdf
Timeline of changes taking place (key milestones) Back to home House of Commons Royal Assent House of Lords LAs commission Local Healthwatch organisations LAs commission NHS complaints advocacy svcs Healthwatch England Local Healthwatch Publish transition plan Action Learning Network for LINks and HealthWatch pathfinders Network of early implementers announced Ongoing devt of early implementers for H&WBBs + sharing the learning Shadow H&WB Boards Local H&WB boards Ongoing development of shadow H&WB Boards and sharing the learning Shadow running of NHS commissioning board NHS Commissioning Board Ongoing development of GP consortia pathfinders and sharing the learning GP Consortia Monitor as new economic regulator Licensing regime fully operational All NHS Trusts become FTs PCT ‘clusters’ to discharge statutory responsibilities whilst supporting emerging GP Consortia Ongoing work of PCT ‘clusters’ SHAs abolished (July 2012) PCTs abolished Public Health consultation ends Public health budgets allocated to LAs Public Health England
Role of the NHS Commissioning Board The NHS Commissioning Board will be accountable to the Secretary of State for managing the overall commissioning revenue limit and for delivering improvements against a number of measures of health outcomes. The Board will in turn hold consortia to account for their performance. The NHS Commissioning Board will: • Provide national leadership on commissioning for quality improvement, for instance by developing commissioning guidelines based on quality standards and by designing tariffs and model NHS contracts. • Promote and extend public and patient involvement and choice • Ensure the development of consortia and hold them to account for outcomes and financial performance • Commission certain services that are not commissioned by consortia, such as the national and regional specialised services • Allocate and account for NHS resources • Work with Monitor to ensure commissioning decisions are fair and transparent and competition is promoted Back to home NHS Commissioning Board information taken from: Equity and Excellence: Liberating the NHS http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_117794.pdf 10
Back to home National Institute for Health and Clinical Excellence (NICE) • NICE is mentioned within all of the consultation documents and within “report of the arm’s length bodies review” its role is described as “Provides national guidance on the promotion of good health and the prevention and treatment of ill health”. It is also recommended to be retained and put its advisory function on a firmer statutory footing by establishing it in primary legislation with an expanded scope to include social care standards. • Commissioners will draw from the NICE library of standards as they commission care. GP consortia and providers will agree local priorities for implementation each year, taking account of the NHS Outcomes Framework. NICE quality standards will be reflected in commissioning contracts and financial incentives. Together with essential regulatory standards, these will provide the national consistency that patients expect from their National Health Service. • Progress on outcomes will be supported by quality standards. These will be developed for the NHS Commissioning Board by NICE, who will develop authoritative standards setting out each part of the patient pathway, and indicators for each step. NICE will rapidly expand its existing work programme to create a comprehensive library of standards for all the main pathways of care. The first eight quality standards – including dementia and depression in adults, have been published. A further five are currently in development and within the next five years, NICE expects to have produced 150 standards. Information on NICE quality standards can be found at: http://www.nice.org.uk/aboutnice/qualitystandards/qualitystandards.jsp 11
Back to home Public Health England Subject to passage of the Health and Social Care Bill, Public Health England will be created in 2012 as part of the Department of Health. This will strengthen the national response on emergency preparedness and health protection, taking over the functions and powers from the Health Protection Agency and the National Treatment Agency for Substance Misuse. Public Health England is part of the Government’s proposals to develop a radical new approach that will empower local communities, enable professional freedoms and unleash new ideas based on the evidence of what works, while ensuring that the country remains resilient to and mitigates against current and future health threats. Public Health England will: • bring together a fragmented system • do nationally what needs to be done • have a new protected public health budget • support local action through funding and the provision of evidence, data and professional leadership. Information taken from: Healthy Lives, Healthy People: Our strategy for public health in England http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_122347.pdf
Back to home Care Quality Commission • In relation to the NHS the Care Quality Commission will, together with Monitor, operate a joint licensing regime. The Care Quality Commission and Monitor already have a duty of co-operation in primary legislation to work closely together to ensure that the regulatory burden of multiple licences is reduced, whilst ensuring robust and proportionate regulation. In due course it is possible that the Care Quality Commission could take on responsibility for a broader range of licensing functions. • The Care Quality Commission will continue to inspect providers against essential levels of safety and quality in a targeted and risk-based way, taking into account information it receives about a provider. This information will come through a range of sources including patient feedback and complaints, HealthWatch England, GP consortia and the NHS Commissioning Board. Where inspection reveals that a provider is not meeting essential levels of safety and quality, the Care Quality Commission will take enforcement action to bring about improvement. • HealthWatch England, a new independent consumer champion from April 2012, which will be an advocate for patients’ rights and concerns, will be constituted as a statutory committee of the Care Quality Commission and will enjoy the benefits of the Care Quality Commission’s independence and scale of operations, including avoiding duplicating work on the assessment of public opinions on health and care issues. CQC information taken from: Liberating the NHS: Legislative Framework and Next Steps http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_122707.pdf 13
HealthWatch England To ensure that local health and care services are truly centred around what matters to those who use them, or may use them in future, the public and patient voice needs to be strengthened. One key element of realising the visions for the NHS, public health and adult social care is the establishment of a new consumer champion, HealthWatch. In summary HealthWatch England will: Be independent of Government through its constitution as a statutory committee of the Care Quality Commission (CQC) Have a chair that will be a non-executive director of the CQC Have its own identity within the CQC Be able to utilise CQC’s expertise and infrastructure HealthWatch England will: Provide leadership, support and advice for local HealthWatch organisations, creating greater consistency across the country Be able to advise the Secretary of State for Health, the NHS Commissioning Board, English local authorities and Monitor as well as the CQC about concerns raised by local HealthWatch organisations Be able to request that the CQC carries out an investigation if it has evidence of poorly performing services. With these responsibilities, Healthwatch will have real power to influence how NHS and social care services are run. HealthWatch England will be able to ensure that people’s concerns about services are brought together and acted on nationally. Back to home HealthWatch information taken from: HealthWatch Transition Plan:http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_125582 14
Monitor Monitor will remain an independent non-departmental public body. Monitor’s overarching duty will be to protect the interests of patients (and other service users) in the provision of health and adult social care by promoting competition where appropriate and through regulation where necessary. In performing this duty, Monitor must promote economy, efficiency and effectiveness in the provision of services. Monitor will also have explicit duties to: • Have regard to the need to promote research and investment by providers, and to the need to secure continuous improvement in the quality of services. • Make effective arrangements to manage potential conflicts between its functions- particularly between economic regulation and its remaining role over FTs. • Have a duty to consult when developing the first set of general license conditions (those conditions that will apply to all licensed providers or all providers within a defined category). This will include a specific requirement to consult the Secretary of State, the NHS Commissioning Board, CQC and HealthWatch England. • Co-operate with the CQC, over and beyond the new duty of partnership for non-departmental bodies. In addition, Monitor will have powers to: • Enforce providers’ licence conditions. • Levy licensing fees on providers – specifically to cover the costs of licensing functions. Monitor information taken from: Liberating the NHS: Legislative Framework and Next Steps http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_122707.pdf Continued on next page
Back to home Monitor’s core functions as Economic Regulator (from April 2012) Licensing Providers Regulating Prices Promoting Competition Supporting Continuity Setting general conditions for all Providers Setting special conditions for individual providers Setting prices where necessary Preventing anticompetitive conduct Additional regulation to ensure continuity Special Administration Enforcement Using prices to improve efficiency Carrying out market studies Advising on competition Collecting and publishing information to deliver functions (price setting, supporting choice etc) 16
Office of Fair Trading • Public services are increasingly being opened up to the private and voluntary sectors with a view to achieving more innovation, diversity and responsiveness to public need. As well as traditional supply side issues, such as avoiding excessive market power, attention is now being focused on demand side issues. This is particularly relevant in opening up markets such as education and healthcare to ensure consumers can play an active role and drive competition. • Related to the opening up of markets to competition, such as Choice and competition in public services, Government in markets and Competitive neutrality, OFT are currently in the process of examining the effect of public sector commissioning and procurement on competition in markets. • OFT will be working with other Government departments to advise on aspects of the public sector reform agenda to ensure that emerging policy does not have an adverse impact on competition. Office of Fair Trading information taken from: Office of Fair Trading Annual Plan 2011-12:http://www.oft.gov.uk/shared_oft/about_oft/ap12/oft1294.pdf Continued on next page
Role and relationship with between the Office of Fair Trading and other organisations within regulation Back to home Role of NHS Commissioning board Role of Monitor Role of Other Organisations • Promoting patient choice • • Deciding how to introduce • choice of any willing • Provider • • Developing standard NHS • Contracts • • Establishing guidance on • commissioning and • procurement • • Assessing complaints on • commissioning / • procurement • Setting and enforcing licence • conditions to prevent anti‐ • competitive behaviour / • facilitate development of • competition • • Investigating anti‐competitive • conduct under Competition Act • 1998 • • Carrying out studies and • referring malfunctioning • markets to the Competition • Commission • • Investigating complaints about • commissioning after referral to • NHS Commissioning Board • • Providing advice to • Government and NHS • Commissioning Board • on barriers to competition / • level playing field • Secretary of State sets • mandate for NHS • Commissioning Board • • OFT has concurrent powers • to investigate anticompetitive • conduct under Competition Act • 1998 • • Competition Commission • investigates barriers to • competition in markets • following reference • • OFT and Competition • Commission investigate and • prevent anti‐competitive • mergers Information taken from: Liberating the NHS, Regulating Healthcare Providers:http://www.dh.gov.uk/en/Consultations/Closedconsultations/DH_117782 18
Developing a Commissioning Outcomes Framework The NHS Commissioning Board will work with clinicians, patients and the public at every level of the system to develop the NHS Outcomes Framework into a more comprehensive set of indicators. The NHS Outcomes Framework will be translated into a commissioning outcomes framework for GP consortia, to create powerful incentives for effective commissioning. It is proposed that the NHS Commissioning Board, supported by NICE, will develop a commissioning outcomes framework so that there is clear, publicly available information on the quality of healthcare services commissioned by consortia, including patient-reported outcome measures and patient experience, and their management of NHS resources. The framework would also seek to capture progress in reducing health inequalities Back to home Commissioning Outcomes Framework information taken from: The NHS Outcomes Framework 2011/12 http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_123138.pdf And Equity and Excellence: Liberating the NHS http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_117794.pdf 19
Mental Health National and Regional Specialist Commissioning (as defined in Specialised Services Definition Set 3rd Ed, Definition 22) Specialised Services for eating disorders Forensic / Secure Mental Health Services. Specialised Mental Health Services for the Deaf Gender Dysphoria Services Perinatal Mental Health Services (mother and baby units) Complex and/or Refractory Disorder Services. Specialised Services for Asperger’s Syndrome and Autism Spectrum Disorder Tier 4 Severe Personality Disorder Services. Neuropsychiatry Services Tier 4 Child and Adolescent Mental Health Services. Back to home Mental Health Specialist Commissioning information taken from: Third edition of the Specialised Services National DefinitionsSet http://www.specialisedservices.nhs.uk/library/26/Specialised_Mental_Health_Services_all_ages.pdf 20
G.P Consortia GP Consortia will need to work closely with the patients and local communities they serve, including through Local Involvement Networks (which will become local HealthWatch bodies) and patient participation groups, and with community partners. In addition to their responsibilities for registered patients, consortia will be responsible for ensuring the provision of comprehensive emergency services for any person in their area. The specific accountabilities, responsibilities and duties of consortia will be set out through primary and secondary legislation. This will include accountability and responsibility for commissioning healthcare services across a range of clinical or service areas, including: • Community health services (except where part of the public health service) • Maternity services • Elective hospital care • Urgent and emergency care including A&E, ambulance and out-of-hours services • Older people’s healthcare services • Healthcare services for children, including those with complex healthcare needs (except for those specialised services commissioned by the NHS CB) • Rehabilitation services • Wheelchair services • Healthcare services for people with mental health conditions • Healthcare services for people with learning disabilities • Continuing healthcare Continued on next page 21
Back to home G.P Consortia continued… • Consortia may agree to commission some health improvement services jointly with local authorities. This could include, for example, obesity, smoking cessation and drug/alcohol services. In some cases, the NHS CB may be asked to commission a service on behalf of Public Health England and may in turn arrange for consortia to commission the service on its behalf. These arrangements and the detail of the respective responsibilities of NHS and public health commissioners are subject to the outcome of the ‘Healthy Lives, Healthy People: Our strategy for public health in England’ consultation (which ended on 31st March 2011). • Monitoring and improving the quality of healthcare provided through these contracts • Providing oversight, with the NHS Commissioning Board, of healthcare providers’ training and education plans. • Consortia will have a duty to inform, engage and involve the public in identifying needs, planning services and considering any proposed changes in how those services are provided. Where this is likely to result in changes in the configuration of services, consortia will be expected to report on the likely impact of those changes and the impact of public involvement on their commissioning decisions. GP Consortia information taken from: The Functions of GP Commissioning Consortia: A working document http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_125006.pdf
Local Authorities Each local authority will take on the function of joining up the commissioning of local NHS services, social care and health improvement. Local authorities will therefore be responsible for: Promoting integration and partnership working between the NHS, social care, public health and other local services and strategies; Producing in partnership with GP Consortia joint strategic needs assessments and joint health and wellbeing strategies that will inform locality commissioning plans which will be done through the health and wellbeing boards Building partnership for service changes and priorities. There will be an escalation process to the NHS Commissioning Board and the Secretary of State, which retain accountability for NHS commissioning decisions. These functions would replace the current statutory functions of Health Overview and Scrutiny Committees. LAs will have an enhanced role in promoting choice and complaints advocacy, through the HealthWatch arrangements they will commission. LAs will have nationally set targets to improve population health outcomes. They will employ Directors of Public Health, who will be jointly appointed with the Public Health Service. Back to home Local Authorities information taken from: Equity and Excellence: Liberating the NHS http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_117794.pdf 23
Back to home Public Health The Government’s goal is a public health service that achieves excellent results, unleashing innovation and liberating professional leadership – with local government and local communities at the heart of improving health and wellbeing for their populations and tackling inequalities. The Public Health White Paper outlines the cross-government framework that will enable local communities to reduce inequalities and improve health, by: • Empowering local government and communities – with new resources, rights and powers to shape their environments and tackle problems • Taking a coherent approach to different stages of life and key transitions – instead of tackling individual risk factors in isolation • Giving every child in every community the best start in life • Making it pay to work – welfare reform/new jobs/employers as public health champions • Designing communities for active ageing and sustainability • Working collaboratively with business and the voluntary sector through the Public Health Responsibility Deal Directors of Public Health will be the strategic leaders for public health and health inequalities in local communities. Local Authorities will employ Directors of Public Health, who will be jointly appointed with the Public Health Service. Public Health will be part of the NHS Commissioning Board’s mandate, with public health support for NHS commissioning nationally and locally. There will be stronger incentives for GPs so that they play an active role in public health. Information taken from: Healthy Lives, Healthy People: Our strategy for public health in England http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_122347.pdf
Local HealthWatch Local HealthWatch organisations will be funded via local authorities and will be accountable to local authorities for operating effectively and providing value for money. Local authorities will have the responsibility for putting in place different arrangements if a local HealthWatch organisation is not operating effectively. At least one representative of local HealthWatch will sit on the new local authority health and wellbeing boards helping to ensure that the consumer voice is integral to the wider, strategic decision–making across local NHS services, adult social care and health improvement. HealthWatch will give local communities a bigger say in how health and social care services are planned, commissioned, delivered and monitored to meet the health and wellbeing needs of local people and groups, and address health inequalities. It will strengthen the voice of local people and groups, helping them to challenge poor quality services. HealthWatch will have an important role supporting everyone in the community, but particularly those who are vulnerable or often unheard. Local HealthWatch will provide information about health and care services and about the choices people can make. From April 2013 it will provide support for people to complain about the quality of NHS services. Continued on next page
Local HealthWatch continued… It is proposed that: • The role of LINks will evolve to become Local HealthWatch which will have an expanded range of functions • Local HealthWatch will be statutory organisations • Local authorities will commission local HealthWatch with freedom to decide how to do this • The DH will make additional funding available to local authorities to support local HealthWatch • Local HealthWatch will have a seat on the local authority health and wellbeing board, to ensure consumer voice is integral to decision-making • From April 2013, local authorities will commission NHS complaints advocacy from any suitable provider, including local HealthWatch, and the service will be accessed through local HealthWatch. HealthWatch information taken from: HealthWatch Transition Plan:http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_125582 Continued on next page
Back to home Local HealthWatch – continuing LINk functions and acquiring new functions Respected, authoritative, influential, credible and very visible within the community Representing the local voice Strong LOCAL consumer voice on views and experiences to influence better health and social care outcomes Scrutinising quality of service provision Seat on the health and wellbeing board Joint Strategic Needs Assessment and Joint Health and Wellbeing Strategy From 2013/14 Empowering people – helping people understand choice Informing the commissioning decision-making process Providing local, evidence based information
Health and wellbeing boards The core purpose of the new health and wellbeing boards is to join up commissioning across the NHS, social care, public health and other services that the board agrees are directly related to health and wellbeing. All upper tier local authorities will have a statutory duty to establish a health and wellbeing board. At the heart of this role is the development and publication of the joint strategic needs assessment (JSNA). The Government proposes that statutory health and wellbeing boards would have four main functions: • to assess the needs of the local population and lead the statutory joint strategic needs assessment; • to promote integration and partnership across areas, including through promoting joined up commissioning plans across the NHS, social care and public health; • to support joint commissioning and pooled budget arrangements, where all parties agree this makes sense; and • to undertake a scrutiny role in relation to major service redesign In addition, health and wellbeing boards will be required to develop a high level joint health and wellbeing strategy (JHWS) that spans the NHS, social care, public health and could potentially consider wider health determinants such as housing and education. Back to home Health and Wellbeing Boards information taken from: Liberating the NHS: Legislative Framework and Next Steps http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_122707.pdf 28
Joint Strategic Needs Assessment (JSNA) and Health and Wellbeing Strategies A joint strategic needs assessment (JSNA) is an assessment of the health and wellbeing needs of the population in a local area. JSNAs aim to establish a shared, evidence based consensus on key local priorities to support commissioning to improve health and wellbeing outcomes and reduce inequalities. Since 2007 it has been a statutory duty for primary care trusts and local authorities to undertake JSNAs; in future Health and Wellbeing Boards will be required to lead enhanced JSNAs, as well as new joint health and wellbeing strategies (JHWS) which will be informed by the needs and assets identified through the JSNA. This requirement will: Support commissioners to decide on priorities in a more joined-up, effective and efficient way; Provide a coherent single needs assessment for all services which will identify the scope for contributions from a wide range of influences such as housing, economic development, spatial planning etc, through Health and Wellbeing Boards; Strike the right balance between facts and figures about local health and wellbeing, and local views about what should be done, through local democratic accountability and HealthWatch. There will be a new shared statutory obligation on GP-led consortia and the local authority (through the health and wellbeing board, to produce JSNA and JHWS and to commission with regard to them. In doing this, they must consider the use of flexibilities under the NHS Act 2006, such as pooled budgets. The NHS Commissioning Board will also be expected to have regard for both JSNA and JHWS. Back to home Information on Joint Strategic Needs Assessments and Health and Wellbeing Strategies can be found at: http://www.idea.gov.uk/idk/aio/27115491andhttp://www.idea.gov.uk/idk/aio/27014541 29
Foundation Trusts The ambition is to create the largest and most vibrant social enterprise sector in the world. The Government’s intention is to free Foundation Trusts from constraints they are under, in line with their original conception, so they can innovate to improve care for patients. In future, they will be regulated in the same way as any other providers, whether from the private or voluntary sector. As all NHS trusts become foundation trusts, staff will have an opportunity to transform their organisations into employee-led social enterprises that they themselves control, freeing them to use their front-line experience to structure services around what works best for patients. For many foundation trusts, a governance model involving staff, the public and patients works well but we recognise that this may not be the best model for all types of foundation trust, particularly smaller organisations such as those providing community services. Ahead of bringing forward legislation, the Bill proposes options for increasing foundation trusts’ freedoms while ensuring financial risk is properly managed – including: • abolishing the arbitrary cap on the amount of income foundation trusts may earn from other sources to reinvest in their services and allowing a broader scope, for example to provide health and care services; • enabling foundation trusts to merge more easily; and • whether foundation trusts should be enabled to tailor their governance arrangements to their local needs, within a broad statutory framework that ensures any surplus and any proceeds are reinvested in the organisation rather than distributed externally. Continued on next page 30
Back to home Foundation Trusts continued… Within three years, we will support all NHS trusts to become foundation trusts. It will not be an option for organisations to decide to remain as an NHS trust rather than become or be part of a foundation trust and in due course, we will repeal the NHS trust legislative model. A new unit in the Department of Health will drive progress and oversee SHAs’ responsibilities in relation to providers. When the new systems is fully established, the Office of Fair Trading (OFT) and the competition Commission will be the sole organisations with responsibility for investigating mergers in health and social care services. For the avoidance of doubt the Bill will make it clear that mergers between Foundation Trusts should be subject to the OFT and the Competition Commissions merger controls from April 2012 onwards Information from: Liberating the NHS: Legislative Framework and Next Steps http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_122707.pdf
Back to home General Practitioners The intention is to put GP commissioning on a statutory basis, with powers and responsibilities set out through primary and secondary legislation. As ‘relevant contractors’ as defined under the NHS Act 2006, all GPs will be required to be a member of a commissioning consortium. Within the new legislative framework, practices will have flexibility to form consortia in ways that they think will secure the best healthcare and health outcomes for their patients and locality. The NHS Commissioning Board will have a duty to ensure comprehensive coverage of GP consortia, and we envisage a reserve power for the Board to assign practices to consortia if necessary. Consortia will be formed on a bottom-up basis, but will need to have sufficient geographic focus to be able to agree and monitor contracts for locality-based services (such as urgent and emergency care), to have responsibility for commissioning services for people who are not registered with a GP practice, to commission services jointly with local authorities, and to fulfil effectively their duties in areas such as safeguarding of children. The consortia will also need to be of sufficient size to manage financial risk effectively, notwithstanding their ability to work with other consortia to manage financial risk. 32