Download
1 / 27
270 likes | 481 Views
Paediatric Head Injury. Head injury is common. USA: 0.2-0.4%, UK 1 million HI presentations pa E/W: 8 sev, 18 mod, 280 mild HI per 100,000 pa UHW 6624 HI patients in 2004 About 50% are paeds Scotland: 4% of under 5s attend A&E pa Edinburgh sick kids: 12 “resus” HI pa.

E N D
Head injury is common • USA: 0.2-0.4%, UK 1 million HI presentations pa • E/W: 8 sev, 18 mod, 280 mild HI per 100,000 pa • UHW 6624 HI patients in 2004 • About 50% are paeds • Scotland: 4% of under 5s attend A&E pa • Edinburgh sick kids: 12 “resus” HI pa
Head injury can be nasty • 40-50% of trauma deaths are mainly attributable to HI • 7% of “Mild” HI have later behavioural problems?
Classifications • Mild GCS 14-15 (80%) • Moderate GCS 9-13 (10%) • Severe GCS 3-8 (10%) • Anatomy: scalp, skull, brain • Focal vs Diffuse • MOI: Blunt vs penetrating • Path: Primary vs Secondary Brain Injury
Anatomical • Scalp: abrasions, haematomas, lacerations • Skull • Vault (?depressed), Basal • Brain • Focal Contusion coup, contrecoup Haematoma subdural, intracerebral extradural (90% adults c #, 70% kids) • Diffuse Concussion DAI
Secondary HI is preventable • Hypoxia • Hypovolaemia • (NB: open fontanelles, large scalp lacerations) • Raised ICP • Blood, oedema, infection • Hypoglycaemia, hypothermia, pyrexia, fits
Pathophysiology • ICP • Normally about 10 mmHg • Higher, worse outcome • CBF • Normally about 50 ml/100g/min • EEG disappears at about 20 • CPP = MAP – ICP • Munro-Kellie
So prevent it! • Oxygen • Treat shock • Image appropriately • Admit appropriately • Refer appropriately
APLS/ATLS Assessment • AVPU/GCS/PERL AMPLE/MIST • Lacs, haems, palpate for depressed # • Fontanelles • Ear/nose CSF/blood, Panda/Battle signs • CNS – focal signs, fundi • Other injuries (especially c-spine), ?NAI
Relevant history • MOI • Clinical progression • Presenting complaints • LOC, Amnesia, Vomiting, Fits, Visual deficits • Warfarin • Alcohol/drugs • Social circs
APLS/ATLS Resus + • ABC! • GCS < 9 needs RSI and normocapnia • Sudden deterioration: • 20% Mannitol 5ml/kg • Aim at MAP 90 mmHg • IV morphine in ventilated patient (?) • Treat seizures as per APLS
Imaging – obs only? • Oriented No # 1/6000 Intra Cranial Haematoma # 1/30 (ie, risk x 200) • Disoriented No # 1/120 # ¼ (ie, risk x 30) • BUT these figures are for adults • 50% of children who die of HI have no # evident
Imaging – modality? • SXR • Misses up to 50% of # • No “brain” information • CT • Radiation = 40 x SXR (1 year’s background) • Sedation • Interpretation • Expense • MRI? Ultrasound?
GCS <13 or E2 GCS 13-14 but not improved at 4 hrs GCS falling New or progressive focal signs Xray or clinical evidence of any # GCS 15 but: fitted, severe HA, N/V, irritable, tense fontanelle GCS 13-14 GCS 15 but non-trivial MOI, LOC, amnesia, vomited, full thickness scalp lac, inadequate history Or if CT should be done but isn’t! Imaging –SIGN guidelines ‘00CT vs SXR
GCS < 14 Focal signs Fit (focal or long) ? Depressed # ? Penetrating/basal # (possibly delayed) LOC > 5 min Amnesia Persisting symptoms HA, V, lethargy Haemophilia Warfarin Ehlers-Danlos Imaging – Edinburgh ’01 Immediate CT vs Obs +/- CT
Imaging – Edinburgh ‘01 • SXR only for < 1 year, with visible HI • LOC per se is not a reason to image (admit and observe only) If children go off, it’s within 5 hours Most vomiting immediately post-HI is “migrainous”, and in 24 hrs post-MI is viral
Admission - SIGN • GCS<15 • Abnormal neurology; seizure at any time • Persisting HA/nausea/vomiting/>5’PTA • Xray or clinical # or penetrating injury • Irritable/abnormal behaviour • Difficulty making full assessment • Medical or social reasons, inc WARFARIN • For children: any LOC, any suspicion NAI
Triage, Assessment, Investigation and Early Management of HI in Infants, Children and Adults More CTs, fewer admissions? Cost neutral??!! Algorithms • Referral from Telephone health advisers • Referral from Community medical services • Selection of patients with HI for CT Head • Selection of patients with HI for C Spine xray
GCS < 13 at any time GCS < 15 at 2 hrs Focal deficit or Fit ? Dep./open/basal # > 1 vomit (discretion!) LOC/amnesia AND Coagulopathy Dangerous MOI > 30 min antegrade Anyone else with any LOC/amnesia (to get CT within 8 hours of injury!) SXR if CT unavailable (Patients to ask why!) SXR as part of skeletal survey in ?NAI NICE ’031 hr vs 8 hr CT
So what should we do?! • SXR probably not so useful in paeds if you’re going to admit the child anyway • SXR still has role in ?NAI • SXR in adults still has use, even with NICE • SIGN was “pragmatic” – only do CT if >10% chance of finding something • NICE is “ideal”
NICE - Admission • Clinically significant abnormality on CT • GCS still not 15 after CT • Meets criteria for scan, but CT unavailable • “Continuing worrying signs of concern to the clinician” (eg, vomiting, severe HA) • “Other sources of concern” (eg, drugs,other injuries, ?NAI, meningism, ?csf leak)
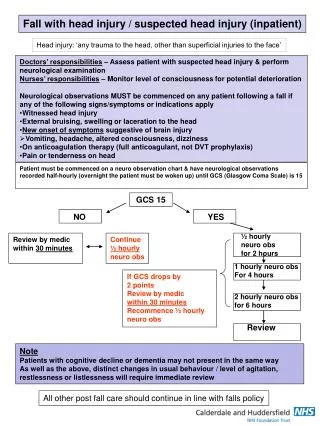
NICE – Obs • GCS, pupils, limbs, RR, HR, BP, T, SpO2 • Minimum frequency for those with GCS 15: • Half hourly for 2 hours • Then hourly for another 4 hours • Then 2 hourly thereafter • If GCS deteriorates then revert to half hourly obs • Only units with staff experienced in paeds HI obs
NICE – Reappraisal • Becomes agitated or behaviour abnormal • Sustained (>30’) fall in GCS (esp. motor) • Any fall in GCS > 2 • Develop severe or increasing HA or persistent vomiting • New or evolving neuro signs Get CT!
NICE – Referral to neurosurgeon “Significant” lesion on scan (surgical definition) OR: Regardless of imaging discuss if : • GCS < 9 after initial resus • Unexplained confusion >4 hours • Deterioration in GCS after admission (motor response) • Progressive focal signs • Seizure without full recovery • Definite or suspected penetrating injury • CSF leak
NICE - Discharge • GCS 15, no continuing worries • Verbal and written advice • Parental supervision • GP follow up within 1 week for all those scanned or admitted, with letters to GP, community paed, school MO, HV…
NICE hand-outs • HI imaging flowchart (NICE, SIGN) • C-spine imaging flowchart (NICE) (NB – no need for peg views and only exceptional need for CT in under 10s) • Paeds GCS • Discharge leaflets • HI proforma
Resources • www.sign.ac.uk • www.nice.org.uk • www.trauma.org