Download
1 / 34
340 likes | 345 Views
Smoking, lipids and lifestyle. Dr Shirley Copland Associate Specialist. Normal heart and coronary artery. Diseased coronary artery. Diabetes and cardiovascular risk. Adults with diabetes have a reduced life expectancy of some 5-10 years Most deaths are due to circulatory diseases

E N D
Smoking, lipids and lifestyle Dr Shirley Copland Associate Specialist
Diabetes and cardiovascular risk • Adults with diabetes have a reduced life expectancy of some 5-10 years • Most deaths are due to circulatory diseases • Heart attacks rates are 3 -5 fold increased • Stroke risk is increased 2-3 fold • After 15 years duration of type 2 diabetes more than 20% of patients have had a heart attack ( UK prospective diabetes study)
AGE DIABETES 45-54 24.8 55-64 37.9 65-74 40.5 Incidence of MI per 1000 women NO DIABETES 4.3 12.6 22.6 DIABETES AND CARDIVASCULAR DISEASE
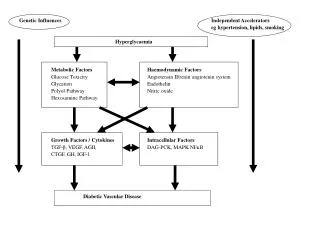
Why the excess risk in Diabetes ? • Thought that raised blood glucose levels are toxic to the lining of blood vessels • Vessels are then more susceptible to damage from all the other risk factors e.g. high blood pressure, smoking • Low density lipoprotein (LDL) is more densely packed with triglyceride which is more readily taken up into the vessel walls causing atheroma plaques
Modifiable Smoking High blood pressure Cholesterol levels Excess weight Lack of exercise High glucose levels Unmodifiable Being male * Family history Age Diabetes mellitus Proteinuria Coronary Risk Factors
Risk Factors - Smoking • Widely recognised to accelerate coronary artery disease and to increase risks of certain cancers • Smoking >20 per day more than doubles the risk of coronary disease • Scottish Diabetes Survey 2004 showed 18% patients with diabetes in Grampian remain smokers
Risk Factors - Smoking • Simple advice to stop smoking has a small but significant effect • Nicotine replacement therapy can double quitting success rates • Zyban also helps more people to be successful but can increase the BP • No definite evidence for benefit of acupuncture • Many people need several attempts to stop –encourage to keep trying! • Monitor for relapse !
Risk Factor - Lifestyle • A 10 kg weight loss in obese patients with diabetes has been shown to reduce mortality by 25% • Exercise helps control weight, blood pressure and lowers blood sugar • In the UK 60-70% of the adult population is considered to be physically inactive • Moderate exercise works - taking a brisk walk most days reduces coronary risk by up to 50%
Risk Factors - Cholesterol • Cholesterol is essential in the body • Component of all cell membranes, needed for manufacture of steroid hormones, used to make bile salts which are necessary for digestion • Excess dietary saturated fat increases blood lipids • Liver is involved in cholesterol manufacture
Risk Factors - Cholesterol • Cholesterol is carried in the blood in particles called lipoproteins. • Lab tests report the total cholesterol (TC) and the amounts of the component particles: • HDL ‘the good’ • LDL ‘the bad’ • TC to HDL ratio ‘the ugly’ • In type 2 diabetes the ratio is often raised due to low HDL
How to reduce Cholesterol • We all know the healthy eating messages - reduced saturated fats, more fruit and veg and oily fish - emphasis is on a balanced diet. • Fish oil supplements shown to be cardio-protective in the short term in high risk patients. No long term overall benefits. • Benecol and Flora pro-active margarines do lower the LDL cholesterol - probably beneficial but no long term studies todate.
How to reduce Cholesterol • Weight loss • Exercise • Good blood sugar control • Exclude secondary causes e.g. hypothyroidism • However despite best efforts the cholesterol levels often remain relatively too high
Heart Protection Study 2002/3 • Major recent trial studying >20,000 subjects aged over 40 with vascular disease, hypertension or diabetes • Patients had ‘normal’ cholesterols at entry • In diabetes patients taking simvastatin: • 27% reduction in major coronary events • 25% reduction in strokes • Note - need to treat 100 people for 5 years to prevent 7 events but benefits would accrue
CARDS 2004 • Almost 3000 patients with type 2 DM • Patients had no known vascular disease but had either retinopathy, microalbuminuria, hypertension or were smokers • LDL < 4.14 on entry • Showed atorvastatin prevented 37 vascular events per 1000 people treated for 4 years
Statin drug therapy • Most effective lipid lowering medications • Many large studies have now shown consistent reductions in cardiovascular risks • Do more than just reduce the cholesterol - protect the circulation • Low incidence of side effects in clinical trials
Potential benefits of ‘statins’ • Reduce major coronary events • Reduce stroke risk • Reduce mortality from heart disease • Reduce need for coronary procedures (angioplasty, coronary artery bypass grafts) • Reduce total mortality
‘STATINS’ • Simvastatin, pravastatin, atorvastatin, fluvastatin and most recently rosuvastatin • Act on the liver enzyme (HMG Co A reductase) involved in cholesterol synthesis hence lowering blood levels • Not used in active liver disease • Few drug interactions (but avoid combination with clarithromycin /erythromycin, ketoconazole, antivirals, ciclosporin) • Grapefruit juice avoidance with simvastatin
‘STATINS’ • Few side effects • Most common are GI effects or headache • Rare side effects include muscle or liver inflammation (< 1 in 10,000 patient years) • Liver tests checked before starting treatment and periodically thereafter and patients are advised to report any new muscle pain • Contra -indicated in pregnancy
Guidelines - shifting the goalpost • Grampian Diabetes Guidelines - Feb 2004 • GP contract targets - April 2004 • Joint British Societies 2 - November 2005
Joint British Societies Guidelines (JBS 2) • All patients with diabetes should receive lifestyle advice and lipids monitored • All patients with known vascular disease should be offered statin therapy • For primary prevention if patients with diabetes meet the following criteria then statin therapy should be offered • Treat to a target of TC 4 and LDL 2
Joint British Societies Guidelines (JBS 2) • All patients with diabetes aged 40 years • Patients with diabetes aged 18-39 years who have at least one of: -retinopathy (severe, prolif. or maculopathy) -nephropathy (incl. microalbuminuira) -poor glycaemic control (HBA1c >9%) -hypertension -TC 6 or features of metabolic syndrome -FH of premature IHD
Joint British Societies Guidelines (JBS 2) • Low dose aspirin : • All people with type 2 DM aged 50 years • Younger patients with diabetes with either -more than 10 years duration -treatment for hypertension or -evidence of complications e.g. retinopathy or nephropathy
Mr JD 69 years • Type 2 DM onset 2005 • Ex smoker 1989 BMI 27 HBA1c 6.9% • BP 158/78 • Left calf claudication • No retinopathy MA screen normal • TC 5.2 LDL 2.9 • Rx Metformin
Mr JD 69 years • Encourage activity increase within limits • Update on foot self care and refer to podiatry • Aspirin • Statin - simvastatin 40 mgs • Ace inhibitor as first line anti-hypertensive
Mrs SD 38 years • Type 2 DM onset 2001 • Smoker BMI 33 HBA1c 7.2% • BP 140/86 • Check out assistant • No retinopathy MA screen normal • TC 4.2 LDL 2.3 TRIGs 1.2 • Rx Metformin
Mrs SD 38 years • Smoking cessation support • Reinforce dietary advice • Consider Xenical • ?Exercise class
Mr J S 38 years • Type 2 DM onset 2000 • Ex smoker BMI 35 HBA1c 8.5% • On anti-hypertensive Rx BP 148/78 • Erectile dysfunction 2003 • No retinopathy MA screen normal • TC 4.8 LDL 2.6 • Rx Insulin, metformin, ramipril, sildenafil
Mr J S 38 years • Review advice on weight reduction and activity level • Insulin and metformin • Ace inhibitor and other agent to lower BP • Sildenafil • Statin • Aspirin
Mr AF 49 years • Type 1 DM since 1994 • Non smoker BMI 27 HBA1c 8.5% • BP 128/76 • Fit joiner • No retinopathy MA screen normal • TC 4.3 LDL 2.5 • Rx Basal bolus insulin regime
Mr AF 49 years • Basal bolus insulin regime • Review education • Simvastatin 20 mgs • Aspirin (nearly 50 years)
Miss C D 34 years • Type 1 DM since 1980 • Smoker BMI 27 HBA1c 7.5% • BP 135/78 • Moderate retinopathy • Microalbuminuria present • TC 4.8 LDL 2.7
Miss C D 34 years • Basal bolus regime of insulin • Support re smoking cessation • Ace inhibitor • Statin • Aspirin • Contraception!