Download
1 / 1
10 likes | 92 Views
The Relationships Between Mental Health Disorders and Attention Deficits: An Analysis from Test Data. Patricia C. Post, Psy.D., Licensed Psychologist Gregory R. Anderson, Ph.D. MENTAL HEALTH BY ATTENTION:

E N D
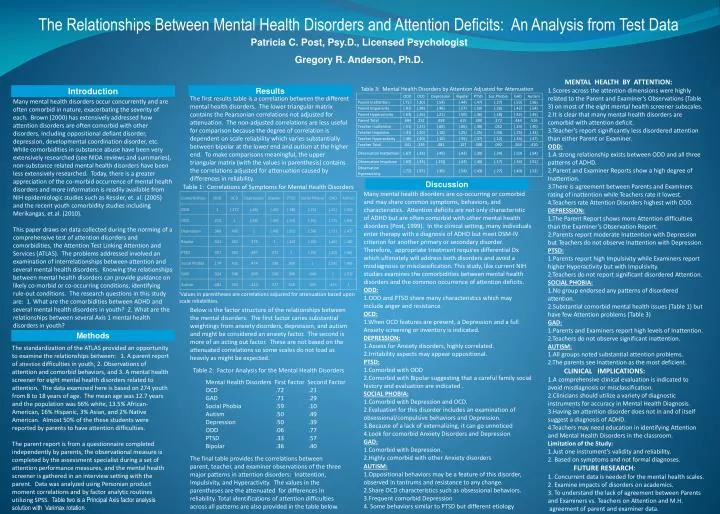
The Relationships Between Mental Health Disorders and Attention Deficits: An Analysis from Test Data Patricia C. Post, Psy.D., Licensed Psychologist Gregory R. Anderson, Ph.D. MENTAL HEALTH BY ATTENTION: 1.Scores across the attention dimensions were highly related to the Parent and Examiner’s Observations (Table 3) on most of the eight mental health screener subscales. 2.It is clear that many mental health disorders are comorbid with attention deficit. 3.Teacher’s report significantly less disordered attention than either Parent or Examiner. ODD: 1.A strong relationship exists between ODD and all three patterns of ADHD. 2.Parent and Examiner Reports show a high degree of Inattention. 3.There is agreement between Parents and Examiners rating of inattention while Teachers rate it lowest. 4.Teachers rate Attention Disorders highest with ODD. DEPRESSION: 1.The Parent Report shows more Attention difficulties than the Examiner’s Observation Report. 2.Parents report moderate Inattention with Depression but Teachers do not observe Inattention with Depression. PTSD: 1.Parents report high Impulsivity while Examiners report higher Hyperactivity but with Impulsivity. 2.Teachers do not report significant disordered Attention. SOCIAL PHOBIA: 1.No group endorsed any patterns of disordered attention. 2.Substantial comorbid mental health issues (Table 1) but have few Attention problems (Table 3) GAD: 1.Parents and Examiners report high levels of Inattention. 2.Teachers do not observe significant inattention. AUTISM: 1.All groups noted substantial attention problems. 2.The parents see Inattention as the most deficient.CLINICAL IMPLICATIONS: 1.A comprehensive clinical evaluation is indicated to avoid misdiagnosis or misclassification. 2.Clinicians should utilize a variety of diagnostic instruments for accuracy in Mental Health Diagnosis. 3.Having an attention disorder does not in and of itself suggest a diagnosis of ADHD. 4.Teachers may need education in identifying Attention and Mental Health Disorders in the classroom. Limitation of the Study: 1.Just one instrument’s validity and reliability. 2. Based on symptoms and not formal diagnoses. FUTURE RESEARCH: 1. Concurrent data is needed for the mental health scales. 2. Examine impacts of disorders on academics. 3. To understand the lack of agreement between Parents and Examiners vs. Teachers on Attention and M.H. agreement of parent and examiner data. Table 3: Mental Health Disorders by Attention Adjusted for Attenuation Introduction Results The first results table is a correlation between the different mental health disorders. The lower triangular matrix contains the Pearsonian correlations not adjusted for attenuation. The non-adjusted correlations are less useful for comparison because the degree of correlation is dependent on scale reliability which varies substantially between bipolar at the lower end and autism at the higher end. To make comparisons meaningful, the upper triangular matrix (with the values in parenthesis) contains the correlations adjusted for attenuation caused by differences in reliability. Many mental health disorders occur concurrently and are often comorbid in nature, exacerbating the severity of each. Brown (2000) has extensively addressed how attention disorders are often comorbid with other disorders, including oppositional defiant disorder, depression, developmental coordination disorder, etc. While comorbidities in substance abuse have been very extensively researched (see NIDA reviews and summaries), non-substance related mental health disorders have been less extensively researched. Today, there is a greater appreciation of the co-morbid occurrence of mental health disorders and more information is readily available from NIH epidemiologic studies such as Kessler, et. al. (2005) and the recent youth comorbidity studies including Merikangas, et.al. (2010). This paper draws on data collected during the norming of a comprehensive test of attention disorders and comorbidities, the Attention Test Linking Attention and Services (ATLAS). The problems addressed involved an examination of interrelationships between attention and several mental health disorders. Knowing the relationships between mental health disorders can provide guidance on likely co-morbid or co-occurring conditions, identifying rule-out conditions. The research questions in this study are: 1. What are the comorbidities between ADHD and several mental health disorders in youth? 2. What are the relationships between several Axis 1 mental health disorders in youth? Discussion Table 1: Correlations of Symptoms for Mental Health Disorders Many mental health disorders are co-occurring or comorbid and may share common symptoms, behaviors, and characteristics. Attention deficits are not only characteristic of ADHD but are often comorbid with other mental health disorders (Post, 1999). In the clinical setting, many individuals enter therapy with a diagnosis of ADHD but meet DSM-IV criterion for another primary or secondary disorder. Therefore, appropriate treatment requires differential Dx which ultimately will address both disorders and avoid a misdiagnosis or misclassification. This study, like current NIH studies examines the comorbidities between mental health disorders and the common occurrence of attention deficits. ODD: 1.ODD and PTSD share many characteristics which may include anger and resistance. OCD: 1.When OCD features are present, a Depression and a full Anxiety screening or inventory is indicated. DEPRESSION: 1.Assess for Anxiety disorders, highly correlated. 2.Irritability aspects may appear oppositional. PTSD: 1.Comorbid with ODD 2.Comorbid with Bipolar suggesting that a careful family social history and evaluation are indicated . SOCIAL PHOBIA: 1.Comorbid with Depression and OCD. 2.Evaluation for this disorder includes an examination of obsessional/compulsive behaviors and Depression. 3.Because of a lack of externalizing, it can go unnoticed 4.Look for comorbid Anxiety Disorders and Depression GAD: 1.Comorbid with Depression. 2.Highly comorbid with other Anxiety disorders ¹Values in parentheses are correlations adjusted for attenuation based upon scale reliabilities. Below is the factor structure of the relationships between the mental disorders. The first factor caries substantial weightings from anxiety disorders, depression, and autism and might be considered an anxiety factor. The second is more of an acting out factor. These are not based on the attenuated correlations so some scales do not load as heavily as might be expected. Methods The standardization of the ATLAS provided an opportunity to examine the relationships between: 1. A parent report of attention difficulties in youth, 2. Observations of attention and comorbid behaviors, and 3. A mental health screener for eight mental health disorders related to attention. The data examined here is based on 274 youth from 8 to 18 years of age. The mean age was 12.7 years and the population was 66% white, 13.5% African-American, 16% Hispanic, 3% Asian, and 2% Native American. Almost 50% of the these students were reported by parents to have attention difficulties. The parent report is from a questionnaire completed independently by parents, the observational measure is completed by the assessment specialist during a set of attention performance measures, and the mental health screener is gathered in an interview setting with the parent. Data was analyzed using Personian product moment correlations and by factor analytic routines utilizing SPSS. Table two is a Principal Axis factor analysis solution with Varimax rotation. Table 2: Factor Analysis for the Mental Health Disorders Mental Health Disorders First Factor Second Factor OCD .72 .21 GAD .71 .29 Social Phobia .59 .10 Autism .50 .49 Depression .50 .39 ODD .06 .77 PTSD .33 .57 Bipolar .36 .40 The final table provides the correlations between parent, teacher, and examiner observations of the three major patterns in attention disorders: Inattention, Impulsivity, and Hyperactivity. The values in the parentheses are the attenuated for differences in reliability. Total identifications of attention difficulties across all patterns are also provided in the table below. AUTISM: 1.Oppositional behaviors may be a feature of this disorder, observed in tantrums and resistance to any change. 2.Share OCD characteristics such as obsessional behaviors. 3.Frequent comorbid Depression 4. Some behaviors similar to PTSD but different etiology