Download
1 / 25
250 likes | 397 Views
PCOS : Menstrual and Metabolic Issues. 2003 Criteria ( 2 out of 3 ) Oligo and / or anovulation Clinical and / or biochemical signs of hyperandrogenism. Polycystic ovaries and exclusion of other etiologies. PCOS – Definition. Revised 2003 Consensus on diagnostic criteria.

E N D
2003 Criteria ( 2 out of 3 ) Oligo and / or anovulation Clinical and / or biochemical signs of hyperandrogenism. Polycystic ovaries and exclusion of other etiologies PCOS – Definition Revised 2003 Consensus on diagnostic criteria Contd…..
Rule out Other Etiologies Congenital adrenal hyperplasia Androgen secreting tumors Cushings syndrome. PCOS – Definition Revised 2003 Consensus on diagnostic criteria
PCOS & Young Girls • PCOS should be considered in any young girl with - Menstrual irregularity - Hirsutism - Obesity • Any of these findings may be the sole feature • May rarely present with - Persistent acne - Scalp hair loss - Hyperhidrosis
Enlarged ovaries More than 10 follicles 2-8 mm in diameter scattered or around periphery Echo dense thickened central stroma Ultrasound Picture of PCOS
PCOS - Anovulatory Symptoms 2/3rd of young girls with PCOS have anovulation and may present with • Oligomenorrhoea • Secondary amenorrhoea • Delayed and heavy bleeding • Lack of premenstrual symptoms e.g. Breast tenderness and dysmenorrhoea
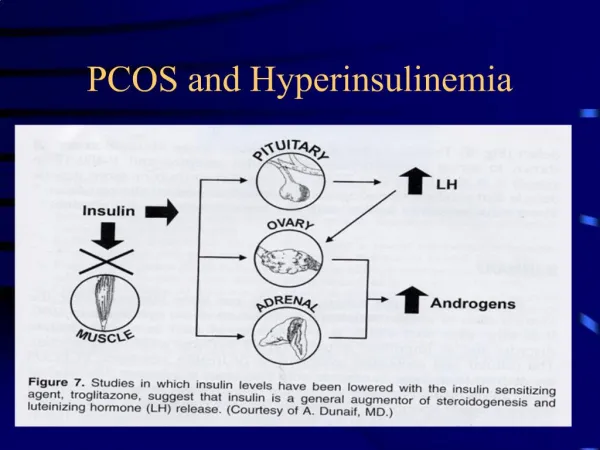
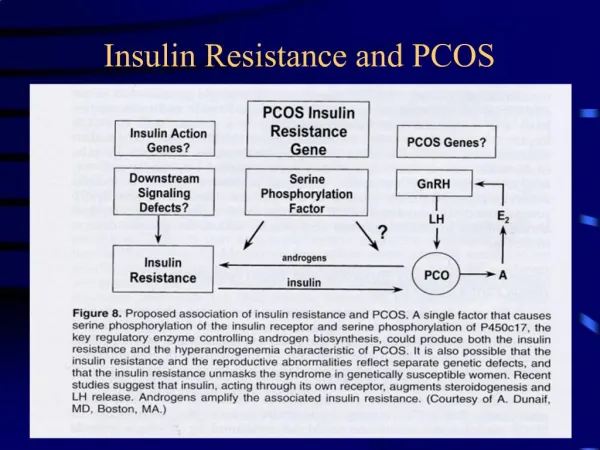
Insulin Receptor Dysfunction Hypothalamus LHRH Pancreas Pituitary Hyperinsulinaemia LH FSH Liver Adrenal Stroma Follicle Elevated DHEAS Elevated Androgens Reduced SHBG Free androgens Hyperinsulinaemia & Hyperandrogenaemia
PCOS Laboratory Diagnosis Initial evaluation • Plasma total testosterone - single most sensitive test for the detection of androgen excess. • Free testosterone • DHEA sulfate - is the main marker of adrenal hyperandrogenism. • Cortisol and thyroid function tests – • are indicated in obese patients to exclude other causes of obesity. • A random cortisol concentration of <10 µg/dL (276 nmol/L) provides evidence against endogenous Cushing
PCOS Laboratory Diagnosis ( contd ) Once a diagnosis of PCOS has been established • A baseline lipid panel • Glucose tolerance test • The fasting glucose concentration is poorly predictive of the two-hour level in PCOS • A two-hour blood glucose greater than 140 mg/dL is presumptive of insulin resistance, which has important therapeutic implications. - Legro, RS, et at Clin Endocrinol Metab 1999
PCOS in Young Girls Treatment strategies include: • Weight loss and exercise • Healthy approach to eating • COC or progestin to testosterone levels and regulate the menstrual cycle • Insulin-sensitizing agents • Antiandrogens • Topical treatment for acne and excess facial hair
Management of Anovulatory PCOS Lifestyle Modification Weight reduction by hypocaloric diet and exercise • insulin sensitivity •LH levels • body fat distribution • circulating androgens • Weight loss by 10 kg resulted in blood glucose, insulin, androstenendione, DHT, E2 levels 29% pregnancy rate in PCOS women - Hollman et al, Human reprod Syn., 1996
Usually is the first line treatment Normalizes androgen levels in 18-21 days Non androgenic progestogens such as desogestrel and levonorgestrel; and anti androgens such as cyproterone acetate are preferred Combination OCP Contd…
Advantages of OC Pill Added advantages of Ethinylestradiol + Antiandrogenic progestin • Suitable for contraception • Favorable effect on Carbohydrate and lipid metabolism • Corrects menstrual cycle disturbances • incidence of anaemia • Frequency of dysmenorrhoea & pelvic inflammatory disease will be lowered • in risk of endometrial and ovarian cancer
Insulin Sensitizors • Metformin • Thiazolidinediones • d-Chiro-inositol
PCOS - Metformin • Oral biguanide antihyperglycemic drug • Used for treatment of non-insulin-dependent diabetes • Category B drug for pregnant women • Metformin lowers blood glucose by • Inhibiting hepatic glucose production • Enhancing peripheral glucose uptake • Enhancing insulin sensitivity at the post-receptor level • Stimulating insulin mediated glucose disposal
PCOS - Metformin • Metformin appears to be very useful in the management of young girls • it suppresses appetite • enhances weight loss • The extended release form of metformin is better tolerated than si the short-acting form. Therapy • Start with 500 mg daily before the evening meal • Can be increased by 500 mg per week • Maximal dose of 2000 mg daily as tolerated - Arslanian, SA, et al J Clin Endocrinol Metab 2002
PCOS - Metformin Range Mean • Menstrual cyclicity 25% - 96% 40% • Reduction in BMI 1% - 4.3% 2.8% • Spontaneous ovulation 30% - 40% • Metabolic Improvements • Test levels. • Insulin levels. ( significant part of beneficial effect due to wt. Loss ) - Glueck, CJ, et al. J Adolesc Health 2001
PCOS - Thiazolidinediones Troglitazone, Rosiglitazone, & Pioglitazone • Increase insulin sensitivity by • Acting on muscle and liver to increase glucose utilization and decrease glucose production • Increase insulin secretion in response to glucose, at least in patients with impaired glucose tolerance. • Their role in management of PCOS is not yet clear. • Troglitazone is not used due to liver toxicity • Rosiglitazone + Pioglitazone not yet extensively evaluated for ovulation induction – ?? less hepatotoxic Nolan, JJ, et al. N Engl J Med 1994
PCOS - D- Chiro-inositol 22 women – D Chiroinositol 1200mg : 6 – 8 weeks 22 women –Placebo Conclusion ; D – Chiroinositol improves ovulation Ref: Nestler et al, New Eng J of Med. April 99
GnRH Agonists • To be used only in exceptional patient who cannot tolerate OCP’s and has persistent heavy bleeding • Patients on long term GnRH agonists should be given low dose estrogen add-back therapy to prevent bone loss during therapy
PCOS – Metabolic Disease linked to Insulin resistance Metabolic Syndrome X • Obesity • Lipid abnormalities • Impaired glucose tolerance • Type 2 Diabetes Mellitus • Hypertension • Hyperuricemia • Higher levels of Plasminogen • Increased coronary artery heart disease
Take Home Message • Is a metabolic disorder • Anovulation may be presenting problem • Treatment is essential • Life style measures (diet and exercise) and Combined oral contraceptive pills are main stay of treatment • Insulin sensitizers play an important role
Concept – Dr. Duru Shah • Contributors Dr. Duru Shah Dr. Sangeeta Agarwal • Editors Dr. Sangeeta Agrawal Dr. Reena Wani
We acknowledge the efforts of our : Coordinators : Dr. Sangeeta Agrawal - Central Dr. Narendra Malhotra - North Dr. Hema Divakar - South Dr. P. C. Mahapatra - East Dr. Uday Thanawala - West In bringing the FOGSI YOUTH EXPRESS to your city.
Charak Pharma Pvt. Ltd CIPLA Ltd. Emcure Pharmaceuticals Ltd GlaxoSmithKline Pharmaceuticals Limited Glenmark Pharmaceuticals Ltd. Metropolis Health Services (India) Pvt.Ltd. Organon India Ltd Roche Pharmaceuticals Ltd. Sandoz Private Limited USV Limited Wyeth Limited This Youth Express has been possible through an educational grant from :