Download
1 / 29
390 likes | 1.04k Views
Menstrual Disorders. Oguchi A. Nwosu M.D. Assistant Profressor Emory Family Medicine Dept. 6/28/07. Menstrual Cycle. Definitions. Menorrhagia Excessive (>80ml) uterine bleeding Prolonged (>7days) regular DUB Abnormal Bleeding, no obvious organic cause usually anovulatory

E N D
Menstrual Disorders Oguchi A. Nwosu M.D. Assistant Profressor Emory Family Medicine Dept. 6/28/07
Definitions • Menorrhagia Excessive (>80ml) uterine bleeding Prolonged (>7days) regular • DUB Abnormal Bleeding, no obvious organic cause usually anovulatory • Oligomenorrhea Uterine bleeding occurring at intervals between 35 days and 6 months • Amenorrhea No menses x at least 6 months Metrorragia, Menometrorrhagia, Polymenorrhea
Ovulatory vs Anovulatory cycles • Anovulatory Oligo or Amenorrhea +/- Menorrhagia • Ovulatory Regular menstrual cycles (plus premenstrual symptoms such as dysmenorrhea and mastalgia
DUB -Defn: Excessively heavy, prolonged or frequent bleeding of uterine origin that is not due to pregnancy, pelvic or systemic disease -Diagnosis of exclusion - Anovulatory -Usually extremes of reproductive life and in pts with PCOS
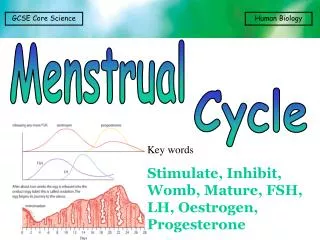
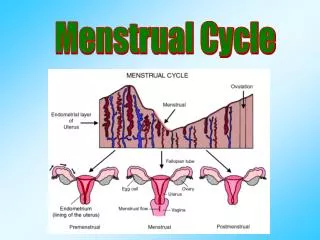
DUB pathophysiology • Disturbance in the HPO axis thus changes in length of menstrual cycle • No progesterone withdrawal from an estrogen-primed endometrium • Endometrium builds up with erratic bleeding as it breaks down.
16year old with daily heavy vaginal bleeding with clots, no cramps • 5ft 7in, 105ibs, normal sec. sex xristics, pelvic normal • Menarche 14, 2 periods last year, heavy lasts 2 weeks, virginal. • I month hx of daily heavy vag bleeding with clots, 8 to 10 pads x day • No associated symptoms • Picture of teenager
DUB management • HCG, CBC, TSH • ? Coagulation workup • Ensure pap smear UTD if appropriate • >35 or Ca risk factors, tamoxifen use – sample endometrium
DUB management • I/V or I/M conjugated estrogen therapy acute DUB--How ?!!!. Usually followed by OCP or progestin • Cyclic progestins for 10 to 12 days each cycle, consider mirena IUD • OCP • D and C – old school, no longer recommended.
Menorrhagia -Heavy vaginal bleeding that is not DUB -Usually secondary to distortion of uterine cavity- heavy with or without prolongation (anatomic). Uterus unable to contract down on open venous sinuses in the zona basalis -Other causes organic, endocrinologic, hemostatic and iatrogenic -Usually ovulatory
5ft’5”, 155Ibs, husband ‘castrated’ Had normal 28 day cycles lasting 5 days Last 1 year or so very heavy periods with clots and occ. ‘flooding’ in the first 3 days with need to use >8pads/day fully soaked, spots for up to 1 week after this. Dysmenorrhea, severe, aching pain lower legs Normal recent pap 40 year old with menorrhagia x 12 months • Picture of middle aged woman
Menorrhagia, Management • History • Physical exam-anemia, obesity, androgen excess e.g. hirsuitism, acne, ecchymosis/purpura, thyroid, galactorrhea, liver/spleen, Pelvic- Uterine, cervical and adnexal
Menorrhagia, management • HCG, CBC, TSH • ? Coagulation workup • Ensure pap smear UTD if appropriate • >35 or Ca risk factors, tamoxifen use sample endometrium Other tests as INDICATED by HX and PE
Menorrhagia, medical management • NSAID’s, 1st line, 5 days, decrease prostaglandins • Danazol, Androgen and prog. competitor , amenorrhea in 4-6 weeks, androgenic side effects • OCP’s, esp. if contraception desired, up to 60% dec. supp. HP axis • Continous OCP’s • Oral continous progestins (day 5 to 26), most prescribed, antiestrogen, downregulates endormetrium • Levonorgestrel IUD (Mirena), High satisfaction rate that approaches surgical techniques • GnRH agonists, Inhibit FSH and LH release– hypogonadism, bone • Conjugated estrogens for acute bleeding • Other treatments as indicated e.g. DDAVP for coagulation defects
Menorrhagia, management summary • Tailor treatment to individual patient. • Consider patients age, coexisting medical diseases, FH, desire for fertility, cost of rx and adverse effects • Surgical management reserved for organic causes (e.g fibroids) or when medical management fails to alleviate symptoms
Amenorrhea, physiologic causes • Male gender • Prepubertal female • Pregnant female • Postmenopausal female
Primary Amenorrhea • Absence of menses by age 14 with absence of SSC (e.g. breast development) or absence by age 16 with normal SSC • Only 3 conditions unique to primary, other causes of amenorrhea can cause either -Vaginal agenesis -Androgen insensitivity syndrome -Turners syndrome (45, X0)
Amenorrhea, causes • Generalized pubertal delay e.g. Turner syndrome • Normal puberty e.g. PCOS • Abnormalities of the genital tract e.g. Ashermans syndrome
Amenorrhea, management • Hx. • PE- These are probably the most important aspects in diagnosis • Remember to always rule out pregnancy • H & P suggests • Ovarian-axis problem- TSH, prolactin, FSH, LH • Hirsuitism-Testosterone, DHEAS, androstenedione and 17-OH progesterone • Chronic ds.- ESR, LFT’s, BUN, cr and UA • CNS- MRI
Amenorrhea, management • If H and P gives no clues to diagnosis-exciting Use step wise approach to diagnosis
Abnormal MenstruationHere’s what you need to remember!! • Always R/O pregnancy, check pap • Try to differentiate anovulatory from ovulatory bleeding • Good history and physical is key( this applies to amenorrhea as well) • Do a focused work up based on your H & P rather than a random set of studies • In amenorrhea, where no indication of cause based on H & P, follow the stepwise algorithm for diagnosis • Know the INDICATIONS for endometrial sampling
References • Slides 25 and 26 courtesy of: Master-Hunter T, Heiman D, Amenorrhea: Evaluation and Treatment. AFP April 15th 2006.