Download
1 / 15
150 likes | 234 Views
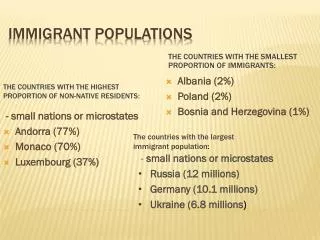
Health Care and Immigrant Populations in the U.S. James A. Litch MD, DTMH Centers for Disease Control and Prevention; WA Department of Health, Epidemiology Office; University of Washington School of Medicine. Presentation Overview. Health issues facing new immigrant populations in the U.S.

E N D
Health Care and Immigrant Populations in the U.S. James A. Litch MD, DTMH Centers for Disease Control and Prevention; WA Department of Health, Epidemiology Office; University of Washington School of Medicine
Presentation Overview • Health issues facing new immigrant populations in the U.S. • One Example: The Tibetan Refugee Resettlement Project • Lessons learned: steps for providers interested in delivering health care to immigrant populations
High Degree of Vulnerability • Disease/Illness • Mental illness • Isolation • Crime • Violence (domestic and community) • Underemployment • Poverty
Health Issues: Immediate • Tuberculosis • Chronic viral hepatitis infection • Intestinal parasites • Nutritional deficiencies • Lack of immunization • Depression and other psychiatric illness
Health Issues: Urgent • Establish primary care and emergency services • Identify chronic medical conditions and treatment alternatives • Language barriers may be persistent
Health Issues: Ongoing New behavioral limits may require rapid change: • Old practices may be dangerous or illegal • The new environment has different risk factors • Awareness of specific cultural practices yields returns
Delivering Health Care • Health conditions may not be the dominant problem patients face • Health care services alone are unlikely to be sufficient • This leads to many challenges that require creative linking of resources
Tibetan Refugee Resettlement Project • Between 1992 and 1993, the first group of Tibetan refugees entered the US • 1000 visas were issued for immigration, but a unique stipulation was made that prevented the use of federal resources for support • This mobilized a nationwide effort in 21 cities
Tibetan Refugee Resettlement Project • Refugees from India, Tibet and Nepal • Came as individuals, with family members to follow in 3-6 years • Seattle received 36 individuals, followed by 150 family members • Tibetan community advocates identified and empowered early after arrival
Tibetan Refugee Resettlement Project • Immigrants were not eligible for public assistance for 1 year • Arrived with a prearranged job offer and household sponsor waiting • Medical screening and care at a Seattle family medicine residency clinic • Structured language, safety/health education, legal support, and acculturation classes • Weekly peer support group
Tibetan Resettlement Project Tibetan Community Program • Key outcome indicator: First group to transition into leadership roles • The program was re-incorporated as a new non-profit organization in 1996 to settle the next larger wave of immigrants
Lessons Learned for Health Care Providers • Specialty or focused clinics for a particular immigrant group are lacking • Travel effort to receive care needs to be appreciated • Language interpreters are NOT optional • Screening is straightforward, but just a starting point
Lessons Learned for Health Care Providers: Cont’d Recognize the need for critical referrals: • English as a second language (ESL) • Counseling/Psychiatric care • Housing • Employment • Establishing residence • Peer support
Steps for Health Care Providers • Commitment is needed from clinic staff, not just the care provider • Training: • Family practice residency training • Diploma in Tropical Medicine and Hygiene • Short-term overseas clinical work • Rotate at a regional international clinics • Get connected in your local community
Conclusion • Mainstream, don’t marginalize • Treat the individual, and the patient • Identify and act to employ outside resources for critical needs