Download
1 / 1
10 likes | 150 Views
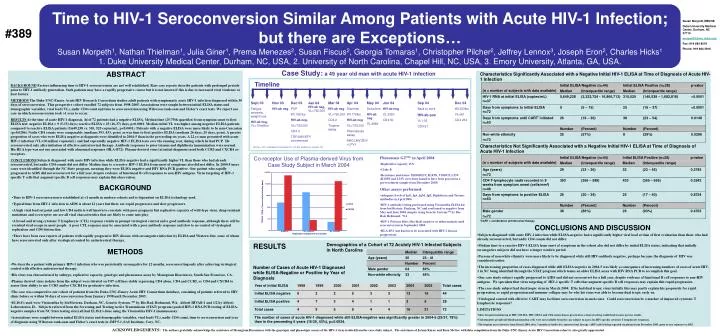
Sept 03 Fatigue, anorexia, weight loss. HIV-ab neg, VL>10million. Nov 03 HIV-ab neg. Dec 03 PCP Wt 185 lbs HIV-ab neg, VL>750,000 CD4 3 TDF/LMV/EFV commenced. Jan 04 HIV-ab neg , VL>750,000. Mar 04 HIV-ab neg VL>750,000 CD4 2 Tropism assay. Apr 04 Diarrhea Wt 178lbs

E N D
Sept 03 Fatigue, anorexia, weight loss. HIV-ab neg, VL>10million Nov 03 HIV-ab neg Dec 03 PCP Wt 185 lbs HIV-ab neg, VL>750,000 CD4 3 TDF/LMV/EFV commenced Jan 04 HIV-ab neg, VL>750,000 Mar 04 HIV-ab neg VL>750,000 CD4 2 Tropism assay Apr 04 Diarrhea Wt 178lbs HIV-ab neg VL>750,000 Phenosense assay ABC/LMV/ZDV+LPV/r May 04 Delusions HIV-ab neg VL 2880 Jun 04 HIV-ab neg VL 2250 CD4 50 Sep 04 Back to work HIV-ab pos VL 135 CD4 57 Dec 04 Wt 233lbs VL<50 CD4 234 Time to HIV-1 Seroconversion Similar Among Patients with Acute HIV-1 Infection; but there are Exceptions… Susan Morpeth1, Nathan Thielman1, Julia Giner1, Prema Menezes2, Susan Fiscus2, Georgia Tomaras1, Christopher Pilcher2, Jeffrey Lennox3, Joseph Eron2, Charles Hicks1 1. Duke University Medical Center, Durham, NC, USA, 2. University of North Carolina, Chapel Hill, NC, USA, 3. Emory University, Atlanta, GA, USA. Susan Morpeth MBChB Duke University Medical Center, Durham, NC 27710 morpe001@mc.duke.edu Fax: 919 684 8519 Phone: 919 684 3916 #389 Case Study: a 49 year old man with acute HIV-1 infection ABSTRACT Characteristics Significantly Associated with a Negative Initial HIV-1 ELISA at Time of Diagnosis of Acute HIV-1 Infection Timeline BACKGROUND Factors influencing time to HIV-1 seroconversion are not well established. Rare case reports describe patients with prolonged periods prior to HIV-1 antibody generation. Such patients may have a rapidly progressive course but it is not known if this is due to increased viral virulence or host factors. METHODS The Duke-UNC-Emory Acute HIV Research Consortium studies adult patients with symptomatic acute HIV-1 infection diagnosed within 30 days of seroconversion. This prospective cohort enrolled 72 subjects from 1998-2005. Associations were sought between initial ELISA status and demographic variables, viral load (VL), nadir CD4 count and time to seroconversion using Wilcoxon rank-sum and Fisher’s exact tests. We report one case in which seroconversion took >1 year to occur. RESULTS At the time of acute HIV-1 diagnosis, 44 of 72 patients had a negative ELISA. Median time (25-75th quartiles) from symptom onset to first ELISA test: negative ELISA = 9 (5-15) days; reactive ELISA = 25 (16-37) days, p<0.0001. Median initial VL was higher among negative ELISA patients compared to reactive ELISA patients (5,649,238 vs. 310, 525 copies/mL, p<0.0001). Patients with a negative ELISA were more likely to be non-Caucasian (p=0.0286). Nadir CD4 counts were comparable (medians 393, 433, p=ns) as was time to first positive ELISA (medians 26 days, 25 days, p=ns). A greater proportion of cases who were ELISA negative at diagnosis were identified in 2004-5 than in the preceeding six years.A 22 yo man presented with acute HIV-1 infection (VL>10 million copies/mL) and had repeatedly negative HIV-1 ELISA tests over the ensuing year, during which he had PCP. He seroconverted only after initiation of effective antiretroviral therapy. Antibody responses to prior tetanus and diphtheria immunization were normal. His HLA type was not one associated with abnormal responses (HLA-B72). Plasma-derived virus (at initial diagnosis) used both CCR5 and CXCR4 co-receptors. CONCLUSIONS Subjects diagnosed with acute HIV infection while ELISA-negative had a significantly higher VL than those who had already seroconverted, but nadir CD4 counts did not differ. Median time to a reactive HIV-1 ELISA from onset of symptoms also did not differ. In 2004-5 more cases were identified through the NC State program, meaning they were ELISA negative and HIV RNA PCR positive. One patient who rapidly progressed to AIDS did not seroconvert for a full year, despite evidence of functional B cell responses to non-HIV antigens. Virus targeting of HIV-1 specific T cells that augment specific B cell responses may explain this observation. Characteristics Not Significantly Associated with a Negative Initial HIV-1 ELISA at Time of Diagnosis of Acute HIV-1 Infection HIV-ab = HIV-1 antibody by Vironostika HIV-1 ELISA, bioMerieux, Durham, NC Co-receptor Use of Plasma-derived Virus from Case Study Subject in March 2004 Phenosense GTTM in April 2004 • Replicative capacity 15% • Clade B • Resistance mutations: M184M/I/V, K103N, V108V/I, L33V (K103N and L33V were later found to have been present in a pre-treatment sample from December 2003) Other assays performed: • Adequate levels of IgG, IgA, IgM, IgE, Diphtheria and Tetanus antibodies in April 2004 • HIV-1 antibody testing performed using Vironostika ELISA kit from bioMerieux, Durham, NC and confirmed as negative from May and June 2004 samples using Genetic SystemsTM by Bio-Rad, Redmond, WA • HIV-1 Western Blots (Bio-Rad) negative or indeterminate until seroconversion in September 2004 • HLA-B72 (not known to be associated with HIV-1 disease progression) BACKGROUND Time to HIV-1 seroconversion is established at <1 month in modern cohorts and is dependent on ELISA technology used. Typical time from HIV-1 infection to AIDS is about 12 years but there are rapid progressors and slow progressors. A high viral load set point and low CD4 nadir is well known to correlate with poor prognosis but replicative capacity of wild-type virus, drug-resistant mutations and co-receptor use are all viral characteristics that are likely to come into play. A broad and strong cytotoxic T lymphocyte (CTL) response results in prompt virological control and a good antibody response, although there will be eventual viral escape in most people. A poor CTL response may be associated with a poor antibody response and slow to no control of virological replication and CD4 destruction. There have been case reports of patients with rapidly progressive HIV disease with seronegative infection by ELISA and Western blot, some of whom have seroconverted only after virological control by antiretroviral therapy. *CART = combination antiretroviral therapy CONCLUSIONS AND DISCUSSION Subject R5 Control X4 Control Subjects diagnosed with acute HIV-1 infection while ELISA-negative had a significantly higher viral load at time of first evaluation than those who had already seroconverted, but nadir CD4 counts did not differ. Median time to a reactive HIV-1 ELISA from onset of symptoms in the cohort also did not differ by initial ELISA status, indicating that initially seronegative subjects did not have a longer window period. Persons of non-white ethnicity were more likely to be diagnosed while still HIV-antibody negative, perhaps because the diagnosis of HIV was considered earlier. The increasing proportion of cases diagnosed while still ELISA negative in 2004-5 was likely a consequence of increasing numbers of cases of acute HIV-1 in NC being identified through the STAT program which teams an older ELISA assay with HIV RNA PCR to accomplish this goal. Our case study subject rapidly progressed to AIDS and did not seroconvert for a full year, despite evidence of functional B cell responses to non-HIV antigens. We speculate that virus targeting of HIV-1 specific T cells that augment specific B cell responses may explain this rapid progression. The case study subject had dual tropic virus in March 2004. If he had dual tropic virus initially this may partly explain his propensity for rapid progression, or rapid progression and immune collapse may be why his virus was able to become dual tropic early on. Virological control with effective CART may facilitate seroconversion in such cases. Could seroconversion be a marker of improved cytotoxic T lymphocyte responses? RESULTS Demographics of a Cohort of 72 Acutely HIV-1 Infected Subjects in North Carolina METHODS We describe a patient with primary HIV-1 infection who was persistently seronegative for 12 months, seroconverting only after achieving virological control with effective antiretroviral therapy. His virus was characterized by subtype, replicative capacity, genotype and phenosense assay by Monogram Biosciences, South San Francisco, CA. Plasma derived virus isolates from the subject were titrated on U87 cell lines stably expressing CD4 alone, CD4 and CCR5, or CD4 and CXCR4 to assess their ability to use CCR5 and/or CXCR4 for productive infection. The case was compared to our cohort of patients from the Duke-UNC-Emory Acute HIV Consortium database, consisting of patients referred to HIV clinic before or within 30 days of seroconversion from January 1998 until December 2005. ELISA’s used were Vironostika by bioMerieux, Durham, NC, Genetic Systems TM by Bio-Rad, Redmond, WA, Abbott HIVAB-1 and 1/2 by Abbott Laboratories, IL. Subjects referred from the Screening and Tracing Active Transmission(STAT) program (pooled HIV-1 RNA PCR testing of ELISA-negative samples from NC State testing sites) all had ELISA’s done using the Vironostika HIV-1 immunoassay. Associations were sought between initial ELISA status and demographic variables, viral load (VL), nadir CD4 count, time to seroconversion and year of diagnosis using Wilcoxon rank-sum and Fisher’s exact tests in JMP 5.1, SAS Institute, Cary, NC. Number of Cases of Acute HIV-1 Diagnosed while ELISA-Negative or Positive by Year of Diagnosis LIMITATIONS • More frequent monitoring of HIV-1 ELISA, HIV-1 RNA and CD4 counts than is practical in a clinical setting would lead to more precise results. • Unfortunately peripheral blood mononuclear cells were not available from the case subject to assess his HIV-specific cytotoxic T lymphocyte responses. • The tropism assay shown is from March 2004, after 3 months of ineffective antiretroviral therapy (ART) and is being repeated on plasma from December 2003, prior to any exposure to ART. ACKNOWLEDGEMENTS: The authors gratefully acknowledge the assistance of Monogram Biosciences with the genotypic and phenotypic assays of the HIV-1 virus isolated from the case study subject. The assistance of JoAnn Kuruc and Kara McGee with data compilation from the Duke-UNC-Emory Acute HIV Consortium cohort is also greatly appreciated.



















