Download
1 / 85
850 likes | 1.07k Views
Methodology Research Group . Evaluation of Potential Mediators in Randomized Trials of Complex Intervention (Psychotherapies). Session 2 Extending Principal Stratification for Characterising Trajectories of Change Richard Emsley. Research funded by: MRC Methodology Grants G0600555

E N D
MethodologyResearch Group Evaluation of Potential Mediators in Randomized Trials of Complex Intervention (Psychotherapies) Session 2 Extending Principal Stratification for Characterising Trajectories of Change Richard Emsley Research funded by: MRC Methodology GrantsG0600555 G0900678, G0800606, G0802418 MHRN Methodology Research Group
More examples of Principal Stratification Introduction to growth curve models Mediation analysis using growth mixture models Latent class trajectory models Outline for session 2
Principal Stratification – SoCRATES example • Considering therapeutic alliance as our mediator/process variable. • We can postulate the existence of two principal strata: • High alliance participants – those observed to have a high alliance in the therapy group together with those in the control group who would have had a high alliance had they been allocated to receive therapy. • Low alliance participants – those observed to have a low alliance in the therapy group together with those in the control group who would have had a low alliance had they been allocated to receive therapy. Frangakis C & Rubin D, Biometrics (2002); Jo B, Psych. Methods (2008).
Principal Strata – SoCRATES example Therapeutic Alliance β α PANSS Randomisation γ Randomisation PANSS High Alliance ITT effect Randomisation PANSS Low Alliance ITT effect
SoCRATES - results Estimated ITT effects on 18 month PANSS Missing data ignorable (MAR) Low alliance High alliance +7.50 (8.18) -15.46 (4.60) Missing data latently ignorable (LI) Low alliance High alliance +6.49 (7.26) -16.97 (5.95)
dX dX U U Sessions Attended Sessions Attended α α β β Randomisation Randomisation Psychotic Symptoms Psychotic Symptoms dY dY Principal Strata – SoCRATES example High Alliance Low Alliance
SoCRATES – effect of Sessions Standard Structural Equation Model Missing data assumption: MAR (uncorrelated errors – no hidden confounding) Low allianceHigh alliance α +14.96 (0.96) +16.91 (0.45) β+0.59 (0.38) -0.75 (0.23) IV Structural Equation Model (with correlated errors – hidden confounding) Low allianceHigh alliance α +14.90 (0.97) +16.95 (0.46) β+0.37 (0.47) -0.80 (0.29) α - effect of randomisation on sessions β - effect of sessions on 18-month PANSS
Mechanisms Evaluation Compliance with allocated treatment Does the participant turn up for any therapy? How many sessions does she attend? Fidelity of therapy How close is the therapy to that described in the treatment manual? Is it a cognitive-behavioural intervention, for example, or merely emotional support? Quality of the therapeutic relationship What is the strength of the therapeutic alliance? Is it associated with the effect of treatment?
Mechanisms Evaluation What is the concomitant medication? Does psychotherapy improve compliance with medication which, in turn, leads to better outcome? What is the direct effect of psychotherapy? Is there any? What is the concomitant substance abuse? Does psychotherapy reduce cannabis use, which in turn leads to improvements in psychotic symptoms? What are the participant’s beliefs? Does psychotherapy change attributions (beliefs), which, in turn, lead to better outcome? How much of the treatment effect is explained by changes in attributions?
Simple example – Two principal strata:Potential Compliers vs Non-compliers Random allocation to treatment or no treatment (control). Those allocated to no treatment cannot get access to therapy. Principal stratum 1: Compliers Treated if allocated to the treatment arm, not treated otherwise. Principal stratum 2: Non-compliers Never receive treatment, regardless of allocation. Possible to identify these two classes in those allocated to treatment; but they remain hidden in the control group.
Simple example – Two principal strata:Potential Low alliance vs Potential High alliance Random allocation to treatment or no treatment. Those allocated to no treatment cannot get access to therapy. Principal stratum 1: Low alliance Treated with low alliance if allocated to the treatment arm, not treated otherwise. Principal stratum 2: High alliance Treated with high alliance if allocated to the treatment arm, not treated otherwise. Possible to identify these two classes in those allocated to treatment; but they remain hidden in the control group.
Simple example – Three principal strata:Non-compliers vs Low alliance vs High alliance Random allocation to treatment or no treatment. Those allocated to no treatment cannot get access to therapy. Principal stratum 1: Non-compliers Never receive treatment, regardless of allocation. Pricipal stratum 2: Low alliance (Partial compliance) Treated with low alliance if allocated to the treatment arm, not treated otherwise. Principal stratum 3: High alliance (Full compliance) Treated with high alliance if allocated to the treatment arm, not treated otherwise. Possible to identify these three classes in those allocated to treatment; but they remain hidden in the control group.
Three principal strata: Compliers vs Always admitted vs Never admitted Random allocation to Hospital admission or Community care. Some of those allocated to Hospital admission never get admitted because of bed shortages. Some allocated to Community care have a crisis and have to be admitted. Principal stratum 1: Compliers Hospital admission if allocated to hospital, Community care, otherwise. Principal stratum 2: Always admitted Hospital admission, regardless of allocation. Principal stratum 3: Never admitted Community care, regardless of allocation. If allocated to Hospital admission and admitted then either Complier or Always admitted. If allocated to Hospital and receive Community care, then Never admitted. If allocated to Community care and receive Community care then either Complier or Never admitted. If allocated to Community care and admitted then always admitted.
Four principal strata based on a potential mediator. Random allocation to CBT or no CBT (control). Those allocated to no CBT cannot get access to therapy. Intermediate outcome – taking antidepressant medication. PS1: take medication irrespective of allocation. PS2: never take medication irrespective of allocation. PS3: take medication only if allocated to CBT. PS4: take medication only if allocated to control. ITT effects in PS1 and PS2 tell us about direct effects of CBT. ITT effects in PS3 and PS3 tell us about the joint effects of CBT and medication.
Principal strata based on remission Participants recruited to the trial during a psychotic episode. Random allocation to CBT or no CBT (control). Those allocated to no CBT cannot get access to therapy. Intermediate outcome –remission of psychotic symptoms. PS1: remission, irrespective of allocation. PS2: no remission, irrespective of allocation PS3: remission only if allocated to CBT. PS4: remission only if allocated to control (PS4 ruled out a priori? – the monotonicity assumption) What if our final outcome is relapse? Only makes sense to look at relapse rates in PS1. No-one to relapse in PS2. No controls for those in PS3. We’ll leave this one for another day!
Notation Zi – treatment group: the outcome of randomisation (Zi=1 for treatment, 0 for controls). Xi′ = X1i, X2i … Xpi – baseline covariates. Yi – observed outcome. Mi – intermediate outcome that is a putative mediator of the effects of treatment on outcome (either a quantitative measure or binary). Ri – response: missing value indicator (Ri=0 if Yi is missing, 1 if observed). We also define the following potential (counterfactual) outcomes: Mi(0) – mediator if randomised to the control condition. Mi(1) – mediator if randomised to treatment.
Principal Strata with a binary mediators • There are now four distinct possibilities (classes) for the joint combination of Mi(1) and Mi(0). • It is sometimes assumed that only one of classes 3 and 4 is present (known as the monotonicity assumption). • Individuals’ class membership is not known: for example, an individual with Zi=1 and Mi=1 is only known to belong to class 2 or class 3.
Principal Strata with a binary mediators • If the mediator is only in the treatment condition (e.g. therapeutic alliance when no intervention offered in the control group), then Mi(0)=0 for everyone. • Classes 2 & 4 do not exist, so we’re only considering the existence of (0,0) and (1,0) classes. • Similar to only thinking about compliers & non-compliers when no active control
Estimation of stratum-specific treatment (ITT) effects Let’s say there are two principal strata, with proportions p1 and p2 (with p1 + p2=1). Let ITTall be the overall ITT effect (which can be estimated directly in the conventional way) Similarly let ITT1 and ITT2be the stratum-specific ITT effects. Then ITTall = p1ITT1 + p2ITT2
The identification problem If ITTall = p1ITT1 + p2ITT2 and we are not prepared to make any further assumptions, then we cannnot get unique estimates of ITT1and ITT2. If we increase ITT1 then ITT2 will decrease to compensate (giving the same value for ITTall). What can we do?
Exclusion restrictions What if stratum 1 corresponds to the Non-compliers? These are participants who never receive treatment whatever the treatment allocation. Let’s assume that allocation also has no effect on outcome in the Non- compliers (an exclusion restriction). Example: If you don’t take the tablets it doesn’t matter whether you have been assigned to the placebo or the supposedly active drug.
With the exclusion restriction we have an identifiable (estimable) stratum-specific treatment effect Now ITTall = p1.0 + p2ITT2 ITTall = p2ITT2 And therefore ITT2 = ITTall/p2 This is the instrumental variable estimator as seen earlier. CACE = Overall ITT effect/Proportion of Compliers
Two exclusion restrictions for the Hospital admission/Community care trial ITTall = p1ITT1 + p2ITT2 + p3ITT3 (p1+p2+p3=1) ITTall = p1ITT1 + p2.0+ p3.0 And therefore ITT1 = ITTall/p1 This is again the instrumental variable estimator (p1 is fairly straightforward to estimate). CACE = Overall ITT effect/Proportion of Compliers
Principal strata based on therapeutic alliance are a problem An a priori exclusion restriction for the Low alliance stratum extremely difficult to justify. In the three-stratum setting there is also a problem unless we can introduce two exclusion restrictions. What is the solution? Answer: Find baseline variables that help predict stratum membership (i.e. help us to discriminate Low and High principal strata). Although they are not necessary for identification, baseline variables that help predict stratum membership are also useful in the presence of exclusion restrictions – they increase the precision of the estimates.
Principal Stratification in Practice Problems: • Imprecise estimates – trials not large enough. • Missing data for intermediate variables (sometimes lots!) – source of imprecision and bias. • Difficult to find baseline variables that are good predictors of stratum membership. • Difficult-to-verify assumptions.
Principal Stratification in Practice • Imprecise estimates – trials not large enough. Combine data from several trials? Meta-regression. Need common outcomes. • Missing data for intermediate variables (sometimes lots!) – source of imprecision and bias. If you think it’s important then collect the data. • Difficult to find baseline variables that are good predictors of stratum membership. Novel designs: Incorporate multiple randomisations to specifically target the intermediate variables. • Difficult-to-verify assumptions. Sensitivity analyses.
Outline for session 2 • More examples of Principal Stratification • Introduction to growth curve models • Mediation analysis using growth mixture models • Latent class trajectory models
Situation considered so far… dX U Mediator Randomisation Outcomes dY
Extending to repeated measures on the outcome variable Time 1 Time 2 Time 3 Mediator Treatment Outcomes Outcomes Outcomes
Simple linear regression where εi is the residual or error term for the ith participant, assumed to be independent of all the residuals for other participants. β1+β2xi is the fixed part of the model εi is the random part of the model We also assume that the variance of Var(yi|xi)= Var(εi|xi)=σ2
Variance Components We split the residual from the first model into two components: ζj is specific to participant j and constant across occasions εij is specific to each participant j at each occasion i ζj is a random effect or random intercept: mean=0, variance=ψ εij is the random deviation of yij from participant j’s mean: mean=0, variance=θ.
Mixed Models • Mixed models are characterized as containing both fixed effects and random effects. • The fixed effects are analogous to standard regression coefficients and are estimated directly. • The random effects are not directly estimated but are summarized according to their estimated variances and covariances.
Stata commands xtmixed - Multilevel mixed-effects linear regression xtmelogit - Multilevel mixed-effects logistic regression Can also use: xtreg - Fixed-, between-, and random-effects, and population-averaged linear models gllamm – Generalised Linear Latent and Mixed Models
Growth Curves for repeated outcome measures • Diagram assumes balanced occasions. • This is the random part of a random coefficient model, which is the same as a traditional linear growth curve model. • Occasion i, subject j Outcome 1 Outcome 2 Outcome 3 1 1 1 1 2 I S
Are missing data a problem? • Are missing data a problem? Why can’t we simply analyse the observed data using an appropriate analysis model? • There are a number of reasons • Invalidity of the estimation method • Loss of precision • Violation of the intention-to-treat principle • Lack of generalisability • The main issue is selection bias.
Missingness mechanisms • Subjects in the sample provide two types of information • The pattern of missing values • The observations actually made • The missing value mechanism is the probability that a set of values are missing given the values taken by the (later) observed and missing observations. • For a number of analysis approaches based on the observed data it will then be possible to specify the MV mechanism or assumptions under which they provide valid inferences.
Rubin’s classification • Rubin’s classification of MV generating mechanisms has proved useful for this purpose • Missing Complete at Random (MCAR) • Missing at Random (MAR) • Not Missing at Random (NMAR)
How to decide between them? • It is not possible to determine empirically which of the three classes we are in • We can never rule out NMAR empirically • Although the data can tell us some things • Can choose between MCAR and MAR • The final decision has to be made on empirical [subject-matter?] as well as theoretical grounds
Some Good News! • Mixed models or random effects models estimated using maximum likelihood estimation is also VALID under the missing at random assumption. • So we can model ALL the data – including the intermediate outcomes. • Ensures participants with some missing values are NOT dropped from the subsequent analysis (as would be performed in SPSS – akin to complete case analysis).
Example: SoCRATES Trial again • We examine the primary outcome, The Positive and Negative Syndromes Schedule (PANSS), an interview-based scale for rating 30 psychotic and non-psychotic symptoms administered blind to condition allocation. • The PANSS was administered • at baseline, • once a week over the first 6 weeks (we just use 6 weeks here) • and then at 3 months, 9 months and 18 months. • In analyses we log transformed the timescale, and considered linear and quadratic terms.
Outline for session 2 • More examples of Principal Stratification • Introduction to growth curve models • Mediation analysis using growth mixture models • Latent class trajectory models
Extending to repeated measures on the outcome variable Time 1 Time 2 Time 3 Mediator Treatment Outcomes Outcomes Outcomes
Principal Strata – with growth curves High Alliance Outcome 1 Outcome 2 Outcome 3 I S Low Alliance Outcome 1 Outcome 2 Outcome 3 I S
Mixture Modelling • Mixture modeling refers to modeling with categorical latent variables that represent subpopulations where population membership is not known but is inferred from the data – such as principal strata. • The simplest longitudinal mixture model is latent class growth analysis (LCGA). In LCGA, the mixture corresponds to different latent trajectory classes. No variation across individuals is allowed within classes. • Another longitudinal mixture model is the growth mixture model (GMM). In GMM, within class variation of individuals is allowed for the latent trajectory classes. The within-class variation is represented by random effects, that is, continuous latent variables, as in regular growth modeling.
Growth Mixture Model • Since c is a categorical latent variable, the interpretation of this GMM is not the same as for a continuous latent variable. • The arrows from c to the growth factors indicate that the intercepts in the regressions of the growth factors on Z vary across the classes of c. Y1 Y2 Y3 Y4 Y5 I S X C Z
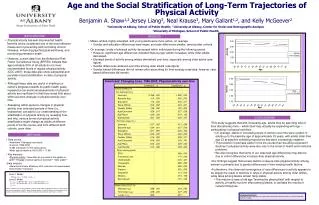
SoCRATES Analysis in MPlus • We simultaneously fit the following models using maximum likelihood: • Principal strata membership on covariates (log of duration of untreated psychosis, centre, years of education) • Quadratic growth curve model within each class, allowing the variances of the intercept • Effect of randomisation on the slope within each class • Bootstrap the procedure to obtain valid standard error estimates.
SoCRATES Analysis in MPlus FINAL CLASS COUNTS AND PROPORTIONS FOR THE LATENT CLASSES BASED ON THE ESTIMATED MODEL Latent Classes 1 69.89513 0.34774 2 131.10487 0.65226 FINAL CLASS COUNTS AND PROPORTIONS FOR THE LATENT CLASS PATTERNS BASED ON ESTIMATED POSTERIOR PROBABILITIES Latent Classes 1 69.89513 0.34774 2 131.10487 0.65226 CLASSIFICATION QUALITY Entropy 0.641