Download
1 / 58
750 likes | 1.46k Views
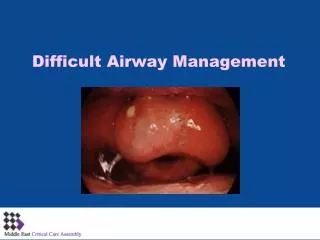
Difficult Airway Management in Anesthesia Part II. Chan Wei-Hung MD Department of Anesthesiology National Taiwan University Hospital. Awake Intubation: Topicalization of Airway. This should be done in such an order: Nasopharynx Oropharynx Vocal cord and trachea.

E N D
Difficult Airway Management in Anesthesia Part II Chan Wei-Hung MD Department of Anesthesiology National Taiwan University Hospital
Awake Intubation: Topicalization of Airway This should be done in such an order: • Nasopharynx • Oropharynx • Vocal cord and trachea Generally speaking, vocal cord and its vincity is the most sensitive site and the most common barrier to successful awake fiberoptic intubation; others are usually tolerable under the spray of local anesthetics.
Sensory Innervations of Airway • Nasal mucosa: sphenopalatine ganglion (V2); anterior ethmoidal nerve (ciliary ganglion) • Oropharynx and supraglottic region: glossopharyngeal nerve • Larynx: superior laryngeal nerve (internal branch) • Trachea: recurrent laryngeal nerve
Drugs to Use • 4% lidocaine with 1:200,000 epinephrine • 4% lidocaine with 0.25~0.5% phenylephrine • Lower concentration of lidocaine makes a slower onset. • Apply bilaterally; wait 2~3 min to take effect.
A Case Report • Intraoperative death of a 21-kg, 4-yr-old boy during bilateral myringotomies and adenoidectomy • Unmeasured amount of 0.5% phenylephrine on the surgical site to control bleeding • BP was 180/110 mmHg and heart rate was 160 beats/min • 2.5 mg labetalol was given • Bradycardia developed, and copious amounts of “pink, frothy fluid” were found from ET tube. • He died 16 h later in ICU. . Anesthesiology 92(3):859-64, 2000
Guidelines for Usage • Phenylephrine for adults should not exceed 0.5 mg or 20 µg/kg in children. • Mild-to-moderate hypertension resulting from phenylephrine use, in a healthy individual, should be closely monitored for 10–15 min before antihypertensive medications • Direct vasodilators or α antagonists are appropriate treatments. • The use of β blockers and calcium-channel blockers should be avoided. • Glucagon may be used to treat β blocker-induced heart failure / pulmonary edema. . Anesthesiology 92(3):859-64, 2000
Lubrication of the Nasal Passage • 7.5 / 7.0 mm nasopharyngeal airway soaked in viscous lidocaine • Determination of the nostril • Determination of the tube size (the bigger the better ?)
Glossopharyngeal Nerve Block 2ml of 1~2% lidocaine each side Aspiration before injection May have the patient in sitting or back-up position 26# spinal needle Advance 0.5 cm into mucosa
Superior Laryngeal Nerve Block • The patient’s neck is slightly hyperextended. • Superior border of lateral wing of thyroid cartilage and greater cornu of hyoid bone are palpated. • Advance the needle just under the greater cornu of hyoid bone until “walk-off” through the firm thyrohyoid membrane, aspirate then inject 1~2% xylocaine 2~3 cc each side.
Transtracheal Injection • The patient’s neck is slightly hyperextended. • Drug : 4% Lidocaine 2 ml or 2% 4 ml (2% needs longer onset time, maybe 10 min) • 22# IV cath, through cricothyroid membrane, 拔掉硬針, 回抽有air bubbles, 噴進去讓病人cough • NPO不夠不可做
Spray As You Go • Inject 0.2-1.0 ml 2~4% lidocaine via suction channel of fiberoscope (esp. near the vocal cord). • Remember to hold the suction tubing when inject. • Wait 30 to 60 sec. Then advance again. • Not as effective as nerve block.
Awake Intubation • Planned or after failed intubation • Fiberoptic intubation • Retrograde intubation • Blind nasal intubation These techniques are essentially not for true emergency situations (time-consuming).
Tube First or Scope First? • ET tube first: • Higher possibility to cause bleeding • Patients feel uneasy with tube in the nasal passage. • Scope first: • Fiberoscope has the chance to divert from midline. • Passage of ET tube through nasopharynx is not assured.
Tube First Technique • Choice of tube size: the size does not matter! • Put the tube in warm water for 5 min • Choice of nostril: left side is preferable • Do not do it forcefully!! (To shift to a smaller ET tube is a virtue.) • Two points of high resistance will be met. • After the second high resistance is passed, advance the tube a little more then hold on. (at about 15 cm) • Turn the tube gently while have the patient breathe deeply, stop at the point of the largest air passage.
Two points of high resistance 1st 2nd 1 st: between turbinate and nasal septum. 2 nd: turning into oropharynx
Advancing the Scope • Always keep the black in the center of the field. (Esp. in distorted anatomy) • Identify the epiglottis. • Pass beneath the epiglottis then bend the scope upwards a little to make the opening of glottis in the center of the field. • Bingo!
Blood: the Most Unwanted • Be gentle in passing the tube through the nasopharynx ! • Suction: not always works well, usually quite unsatisfactory. • Slightly back-up position, have the patient swallowing the blood. • Advance the scope blindly: esophagus is often entered (which means the midline position of the scope is secured), then withdraw slowly. Once the scope slips out of esophagus, glottic opening is hopefully in view.
The Oral Approach • A more curved pathway compared with nasal passage • Less convenient in distorted anatomy • Prone to deviate from midline position (an intubating airway is helpful.) • Easy to cause fiberoscope damage • Can be done at sitting position
The Oral Approach • An oral bite is a must unless very good topical anesthesia (which is a rarity.) • Advance the tip of the scope till the posterior part of the tongue base then bend downwards nearly 90°; epiglottis will appear in view. • Advance between epiglottis and posterior wall of larynx. Glottic opening would be found.
Causes of Failed Fiberoptic Intubation • Lack of expertise (most common) • Secretion and blood • Fogging of lenses • Poor topical anesthesia • Distorted anatomy • Fiberoscope malfunction • Inadvertent passage of fiberoscope through Murphy’s eye
Practice of Fiberoptic Intubation on Healthy Patients More Often !
The Three Tenors: good for the concert, disaster for the OR.
Laryngeal Mask Airway (LMA) Sizes #1 <6.5 kg 2-5 ml 3.5 #2 6.5-20 kg 10 ml 4.5 #2 1/2 20-30 kg 14 ml 5.0 #3 30-60 kg 20 ml 6.0 (cuffed) #4 60+ kg 30 ml 6.5 (cuffed) #5 >70 kg
Does the Size Matter? • It does in routine use. • It dose not in difficult airway management. • In patients with macroglossia, limited mouth opening, poor dentition, enlarged adenoid tissue, insertion of LMA is perceivably difficult; the use of LMA in these cases should be reconsidered. • A smaller size than recommended may help.
The Technique of Insertion (I) • Deflate the mask while pressing the bowl of the LMA against a flat surface. • Lubricate the posterior surface of the LMA. • After induction, patient’s head is slightly extended. • Insert the LMA into patient’s mouth, pressing the back firmly against the hard palate.
The Technique of Insertion (II) • LMA should be seen to flatten against the palate. • Push the LMA further while firmly pressing against the palate. • Once pass the tongue, the LMA can be advanced without resistance. • Inflate the cuff, then check the ETCO2 after several manual ventilation. • Secure LMA with tape, with the black line facing the nose.
Keypoints for Successful LMA Insertion • Practice and expertise • Choice of correct size • Proper patient positioning • Adherence to correct technique • Adequate depth of anesthesia
Removal of LMA • At deep or light level of anesthesia. • Do not suction inside the LMA!
Don’t treat LMA like an ET tube! Don’t push over the posterior pharyngeal wall! Don’t suction inside the LMA!
After LMA Insertion • Awake the patient and cancel operation. • Continue the operation with LMA. • Fiberoscope intubation with LMA (then change to a bigger ET tube).
Contraindications of LMA • Patients at the risk of aspiration • Patients with poor pulmonary compliance • Pharyngeal pathology
Light Wand • Et tube is attached to the light wand after lubrication both inside and outside the tube. • A 90-degree bend is made at the distal end of the tube. • After induction and mask ventilation is assured, put the patient in neutral position with the neck slightly extended. • Open the mouth and apply light wand until light is seen in thyroid cartilage; advance the tube.
Problem Shooting in Light Wand • No light is seen in the neck: • Light malfunction • Increase the length of the bent end • Light is seen in pyriform sinus: • Withdraw-reapply policy
Admonition • LMA and lightwand are basically used for difficult intubation after induction and mask ventilation is assured. • In case of difficult mask ventilation, LMA can be tried in a very short time; shift to cricothyroid membrane puncture ASAP if LMA fails after several attempts. Lightwand is generally not desirable in difficult mask ventilation. • Rethink and take great care when use LMA and lightwand in limited mouth opening!
CO2 waveform in a 10 y/o boy after intubation. Breathing sound: clear bilaterally Anesthesia & Analgesia 66:481, 1987
CO2 waveform during tracheal and esophageal intubation. Anesthesia & Analgesia 73:333, 1991