Download
1 / 38
380 likes | 572 Views
Secondary Causes of Dyslipidemia. Mary-Anne Doyle, MD, FRCPC University of Ottawa October 6, 2014. Objectives. List the secondary causes of: hypercholesterolemia alone, hypertriglyceridemia alone, hypercholesterolemia and hypertriglyceridema and hypoalphalipoproteinemia (low HDL‐C).

E N D
Secondary Causes of Dyslipidemia Mary-Anne Doyle, MD, FRCPC University of Ottawa October 6, 2014
Objectives • List the secondary causes of: hypercholesterolemia alone, hypertriglyceridemia alone, hypercholesterolemia and hypertriglyceridema and hypoalphalipoproteinemia (low HDL‐C). • Identify the main mechanisms involved in secondary hyperlipidaemia seen in hypothyroidism, diabetes mellitus, nephrotic syndrome, chronic renal failure, cirrhosis, cholestasis.
Disease • Diabetes • Hypothyroidism • Obesity • Alcoholism • Renal Failure • Nephrotic Syndrome • Liver Disorders-NASH • HIV • Glycogen Storage Disease • Cushing Syndrome • Acromegaly
Type 1 Diabetes Increased VLDL and chylomicrons Insulin deficiency ↓ Mobilization of FFA from peripheral tissue ↓ Increased VLDL secretion ↓ transcription of LPL gene and decreased LPL activity Administration of insulin restores triglyceride levels to normal within a few days
Type 2 Diabetes • ↑ VLDL • ↑ FFA influx • Increased TG production • ↑ LDL-C • Increased if under poor control • Increase cardiovascular risk
Diabetes Treatment: • Optimize glycemic control/insulin administration • Lifestyle factors • Exercise, weight loss • Medical Therapy • HMG co-reductase inhibitors • Fibrates-gemfibrozil, fenofibrates • Niacin-may aggravate glucose intolerance • Cholestyramine-not generally well tolerated due to GI side effects
Hypothyroidism ↑ LDL-C-Usually mild Mechanism • ↓conversion of cholesterol to bile acids • Down-regulation of hepatic LDL receptors • Decreased hepatic lipase activity • May have increased IDL, and mild ↑ TG • Improves with treatment of hypothyroidism
Obesity Increase in adipocyte mass Decrease in insulin sensitivity Increase FFA to the liver Increased VLDL • ↑simple CHO→hepatic production of VLDL/LDL-C • Low HDL-C –normalizes with weight loss • Metabolic Syndrome: • abdominal obesity • insulin resistance • glucose intolerance • hypertension
Alcoholism • Moderate Intake (i.e. 1-2 ounces/day) • ↑ HDL • ↓ risk of coronary artery disease • Excessive amounts • ↑ TG levels (VLDL/Chylomicrons) • May have underlying genetic pre-disposition • ↑ risk of pancreatitis and atherosclerosis • Adds to obesity- 1 oz EtOH =200 calories
Chronic Renal Failure • Increased TC/LDL-C less prominent. TC/LDL-C often normal or low. • ↑TG • ~30% have hypertriglyceridemia • Enriched with Apo-CIII • Decreased clearance from circulation • Decreased LPL activity and hepatic lipase (mechanism unclear) • Low HDL • Impaired maturation • Down-regulation of LCAT
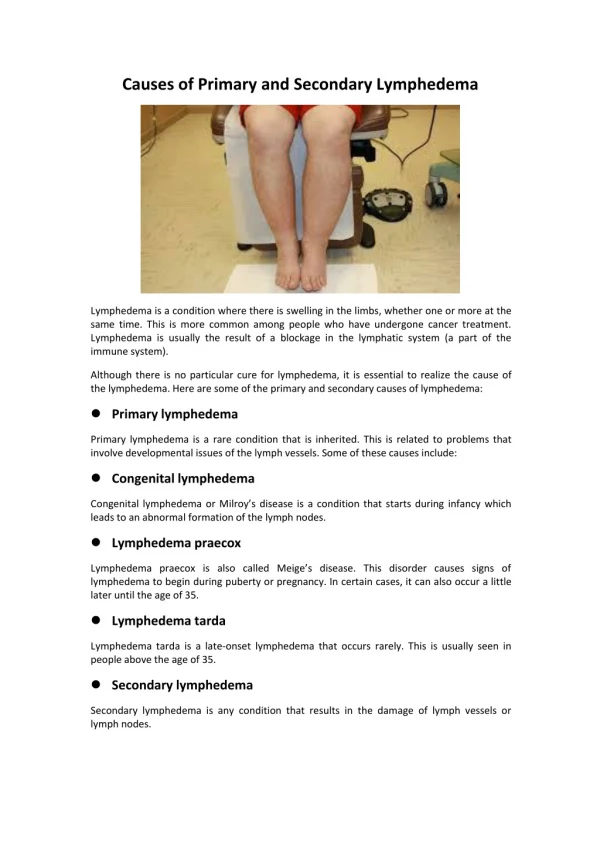
Nephrotic Syndrome • Biphasic based on albumin levels: • Initially increased TC/LDL. • As albumin levels fall -High TC, LDL, TG • Increased hepatic production of lipoproteins due to decreased oncotic pressure • Diminished lipid catabolism • Normal or low HDL • Apo –A1 and Apo-A2 usually normal • Impaired maturation of lipid poor HDL to mature cardioprotective HDL. Mechanism unclear.
Liver Disorders-Cholestasis • Hypercholesterolemia (TC/LDL) common feature • Due to extrahepatic/intrahepatic obstruction • Abnormal lipoproteins: Accumulation of lipoprotein-X (Lp-X) • Not removed by LDL-receptor • Failure to exert feedback on cholesterol synthesis • Athrogenecity unclear • LDL contains unusually large amounts of TG. • Increased TC and LDL correlates with worsening histologic stage • Increased HDL
Cholestasis-Clinical Findings • Plantar Xanthomas-sites of minor trauma/palmar creases • Eruptive Xanthomas may be present • Xanthomatous involvement of nerves→peripheral neuropathy
Liver Disorders Non-alcoholic steatohepatitis (NASH) • Characterized by hepatic steatosis→cirrhosis • Hypertriglyceridemia common • Mechanism unclear • Possibly misdirection from oxidative pathways→hepatic triglyceride synthesis
Glycogen Storage Disorders • Mutation in glucose-6-phosphatase • Inability to mobilize hepatic glucose during fasting ↓ hypoinsulinemia ↓ ↑ release of FFA from adipose tissue ↓ ↑hepatic fatty acid synthesis ↓ ↑ VLDL secretion
Cushing Syndrome • Insulin resistance is present • ↑ VLDL synthesis and ↑ TG • Mild ↑ LDL-C • Becomes more pronounced as insulin resistance progresses to “steroid induced” diabetes
Acromegaly • Mild ↑ TG • 2⁰ insulin resistance
Anorexia Nervosa • Approximately 40% of patients have ↑ LDL-C • Mechanism not clear • Possible due to decreased excretion of bile acids/cholesterol • Lipid levels return to normal when proper nutrition is restored.
HIV • Lipid disorders common in HIV-infected individuals • Multifactorial • HIV infection • Antiviral medications • Body composition • Immune reconstitution • HIV infection is associated with mild increase in TG and VLDL, decrease LDL and HDL. • Thought to be due to decreased clearance of TG and to a lesser extent, increased VLDL synthesis
Medications • Antihypertensives: Diuretics Betablockers • Steroids: Estrogens Progestins Androgens Corticosteroids • Other Cyclosporine Carbamazepine Retinoid HIV Protease Inhibitors
Diuretics • Thiazides • e.g. hydrochlorathiazide • Dose-dependent • Little or no effect at lower doses (i.e. HCTZ 12.5 mg/day) • With initiation of high doses • ↑ VLDL (~50%), ↑ LDL 10-20% • Return to normal with chronic use (i.e> 1 year) • Loop diuretics • e.g. furosemide • Slight increase in VLDL
Beta-Blockers • Varies with pharmacologic properties • Non-selective vs β1 selective, vs α/β combined blockade • May be more prominent in smokers • Non-selective • Propanolol, sotalol, timolol • Increase TG 20-40% • Decrease HDL 10% • β1 selective • Metoprolol • Increase TG 15-30% • Minimal effect on HDL • Intrinsic sympathomimetic activity • Pindolol • minor lipid changes • Combined α/β-blocker • Labetatol • Cholesterol levels relatively unaffacted
Alpha-Blockers • Selective alpha-1 blockers (i.e. prazosin, doxasin and terazosin) have favourable effect on lipids • ↓ TC 3-5%, ↓TG 3-4%
Steroids • Estrogens • Progestins • Androgens • Corticosteroids
Estrogen • Conjugated estrogen (Premarin), transdermal estrogen, oral ethinyl estradiol (OCP) • Increased VLDL and HDL synthesis; slight decrease in LDL-C • ↑ TG (~15%) and ↑ HDL-C • Distinct pattern (usually TG and HDL-C are inversely related)
Estrogen • TG require monitoring when Oral contraceptive therapy or hormone replacement therapy initiated. • Transdermal preparation have less effect due to avoidance of hepatic first pass effect. • LDL-C decreased slightly; coronary vasodilating effect; but increased CV risk in Women’s Health Initiative (WHI) Study
Progestins Postmenopausal hormone replacement • Medroxyprogesteroneacetate - Provera • Cycled with estrogen if no hysterectomy • Eliminates increased risk of endometrial cancer • LDL - increases slightly • HDL - decreases slightly • Blunts beneficial effects of estrogen on lipids
Progestins ORAL CONTRACEPTIVE - 3 main progestins: • levonorgestrel- most reduction in HDL • norethindrone- intermediate • desogestrel- minimal lipid effects; selective progestagen - minimally androgenic • lipid effects depend on progestin dosage • effect of oral contraceptive on CAD risk unclear
Androgens Testosterone • treatment of hypogonal males • oral, intramuscular, transdermal • lipid effects more pronounced when given orally • HDL decreased (mainly HDL2) • LDL slightly increased • VLDL and Chylomicrons decreased Anabolic steroids • misused by athletes • similar to above but more marked effects on lipids
Corticosteroids • Insulin resistance is present • ↑ VLDL synthesis and ↑ TG • Mild ↑ LDL-C • Becomes more pronounced as insulin resistance progresses to “steroid induced” diabetes
HIV Medications • Several HIV medications known to increase TG production/LDL-C • Most commonly due to protease inhibitors • 2-3 fold increase in VLDL production
Other Medications • Retinoids (dermatologic agent): • increased VLDL and chylomicrons • Cyclosporine (immunosuppressant): • increased LDL-C • Carbamazepine (anticonvulsant): • increased LDL-C
Summary • There are many reversible causes of dyslipidemia • Common diseases included diabetes, hypothyroidism, alcoholism, obesity, renal disease, and liver disease • Common medications include antihypertensive agents and gonadal steroids. • Identifying and treating the underlying condition may prevent the need for lipid lowering therapy.