Download
1 / 40
400 likes | 497 Views
What Not To Miss... DM and CV disease 2013. Adam Wolfe, DO Medical Director, Primary Care MHMG IM Residency Director, Metro Health Hospital. Conflicts - none. Game Plan. New targets and role in therapy New cardiovascular data 2013 What not to miss… Comments and questions. Case #1- JM.

E N D
What Not To Miss...DM and CV disease 2013 Adam Wolfe, DO Medical Director, Primary Care MHMG IM Residency Director, Metro Health Hospital
Game Plan... • New targets and role in therapy • New cardiovascular data 2013 • What not to miss… • Comments and questions
Case #1- JM • JM is a 56 year old male with non-insulin requiring DM diagnosed 4 years ago, systolic HF (EF 25%), CAD (post LAD stent 3 years ago), Serum Cr = 1.1mg/dL • Current medications: metformin 850 mg BID, sitagliptin 100 mg daily, valsartan 80 mg BID, carvedilol 12.5 mg BID • A1C 1 month ago was 7.6% • Present BP: 142/86 mm Hg • No signs of retinopathy, + microalbumin on last urinary testing • Based on the above clinical findings, the next most appropriate therapy for the patient’s blood sugar control would be:
Case #1 (cont) • A) Continue present therapy • B) Increase Metformin therapy to 1000 mg twice daily • C) Add basal insulin therapy for FBS goal of 100 mg/dL • D) Initiate Invokana (canagliflozin) • E) Add Avandia therapy at 4 mg daily
Case #1 (cont) • A) Continue present therapy • B) Increase Metformin therapy to 1000 mg twice daily • C) Add basal insulin therapy for FBS goal of 100 mg/dL • D) Initiate Invokana (canagliflozin) • E) Add Avandia therapy at 4 mg daily
New Therapies in DM • Considerations • Clinical efficacy • Weight effect • Hypoglycemia risk • Adverse interactions or effects • Cost • CV safety
FDA mandate on future DM trials • In July 2008, the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee met to discuss the role of CV assessment in the premarketing and postmarketing settings. The FDA determined that concerns about CV risk should be more thoroughly addressed during drug development; their newly issued guidelines will result in profound changes in the ways new antidiabetes drugs are evaluated and brought to market in the future • Continue to evolve safety data • Surrogate endpoints cannot replace large scale clinical trials looking at CV outcomes
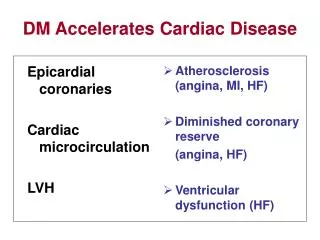
Expanding the physiology of DM in practice New options in therapy
Physiology - natural progression Earlier Diagnosis + Earlier Treatment + Better Options = Better Outcomes Adapted: Nathan DM. N Engl J Med. 2002;347:1342-9
‘Ominous Octet’ DeFronzo R et al. Diabetes. 2009;58:773-795.
Sites of Action Secretagogues Simulate insulin secretion Alpha-glucosidase inhibitors Inhibitcarbohydratebreakdown Incretins • Insulin secretion Glucagon secretion Incretins Slow gastric emptying MetforminThiazolidinediones • Glucose metabolism Thiazolidinediones • Glucose metabolism FFA output MetforminThiazolidinediones Suppress glucose production Saltiel AR, Olefsky JM. Diabetes. 1996;45:1661–1669 Drucker DJ. MolEndocrinol. 2003;17:161–171
canagliflozin (Invokana) • Approved March 29, 2013 • New mechanism of action - SGLT2 inhibition • Dose related A1c reductions studied as monotherapy and in combination with SFU, DPP4, TZD, Basal Insulin • Weight loss associated (2.5-3 kg) and BP reduction • CV outcomes coming…CANVAS (2015)*
Renal Targets Am J Renal Phys 280(1): F10-F18 2001
Mechanism of action – SGLT2 inhibitors • Inhibition of renal tubular Na+ glucose cotransporter reversal of glucose toxicity • Increased insulin sensitivity of skeletal muscle • Increased insulin sensitivity of liver • Decreased gluconeogenesis • Improved beta cell function
Dapagliflozin (Farxiga) • FDA Approval Jan 8, 2014 • 16 trials and over 9600 patients studied • Initially disallowed (2012) due to concerns for bladder malignancy marker • Dose related A1c reductions studied as monotherapy and in combination with SFU, DPP4, TZD, Basal
Clinical concerns… Schernthaner G. et al. Diabetes Care 2013;36:2508-2515
Case #2 - Mary Mary is a 50-year-old woman who was diagnosed with T2DM 5 years ago. After serum Creatinine = 1.4 mg/dL, she stopped metformin and started SFU Past Med History: non-smoker, longstanding hypertension, hyperlipidemia, chronic kidney disease, sleep apnea, and osteoarthritis. Recent LVEF = 45% by echocardiography Family History: Mother died of CHF at age 70, Father died following an MI at age 50 Medications: ASA 81 mg/d, glimepiride 4 mg/d, lisinopril 20 mg/d, simvastatin 40 mg/d On her physical exam, she is obese (BMI: 46.7 kg/m2) and has 2+ pitting edema. Her BP is 126/70 mm Hg. Her laboratory findings include the following: LDL: 90 mg/dL; HDL: 35 mg/dL; triglycerides: 170 mg/dL; HbA1c: 7.5%; creatinine: 1.4 mg/dL. Recent stress echocardiography demonstrated no evidence of ischemia
Which of the following is the next best therapy for Mary? No change – follow-up 3 months Discontinue SFU and re-initiate Metformin therapy Add incretin agent to SFU therapy Decrease SFU and add incretin agent Discontinue SFU and initiate TZD Discontinue SFU and initiate basal insulin therapy
Which of the following is the next best therapy for Mary? No change – follow-up 3 months Discontinue SFU and re-initiate Metformin therapy Add incretin agent to SFU therapy Decrease SFU and add incretin agent Discontinue SFU and initiate TZD Discontinue SFU and initiate basal insulin therapy
HISTORICAL LOOK Safety data
DCCT/EDIC: Intensive glucose control reduces long-term CV risk N = 1441 with type 1 diabetes 0.12 0.12 42% (95% CI 9%–63%) P = 0.02 57% (95% CI 12%–79%) P = 0.02 0.10 0.10 0.08 0.08 Cumulative incidence of any first CV event Cumulative CV death, nonfatal MI, stroke Conventional 52 events 0.06 0.06 Conventional 25 events 0.04 0.04 Intensive 31 events Intensive 11 events 0.02 0.02 0 0 0 5 10 15 20 0 5 10 15 20 Time (years) Time (years) N Engl J Med. 2005;353:2643-53.
Historical Cardiovascular Data • (+) UKPDS – (2008) – 15% reduction in MI and 13% reduction in death in DM2 patients (1) • (-) ACCORD – (2008) – increased all-cause mortality for intensive control group (2) • (~) ADVANCE – (2008) – non-statistical difference of macrovascular events and mortality (3) • (~) VADT – (2009) – non-statistical difference of time to first majory CV event (4) 1. N Engl J Med 2008;359:1577-1589 2- N Engl J Med 2008; 358:2545-2559 3-N Engl J Med 2008; 358:2560-2572 4-N Engl J Med 2009; 360:129-139
alogliptin N Engl J Med 2013; 369:1327-1335
Cumulative Kaplan–Meier Estimates of the Time to tPrimary End-Point Event or Other Safety End Point. N Engl J Med 2013;369:1327-1335
Major Safety End Points. White WB et al. N Engl J Med 2013;369:1327-1335
Final thoughts on alogliptin? • Improved A1C levels and durability in trials • More selective for DPP4 than other agents • No increase in CV events from EXAMINE BMC Endocr Disord. 2013;13(9)
N Engl J Med 2013;369:1317-1326 SAVOR SaxagliptinAssessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus
Kaplan–Meier Rates of the Primary and Secondary End Points. Scirica BM et al. N Engl J Med 2013;369:1317-1326
Prespecified Clinical End Points. Scirica BM et al. N Engl J Med 2013;369:1317-1326
What Not To Miss... • Avandia news – reinstated after readjudication of the RECORD data • Actos in IGT patients (ACT-NOW) • FDA Panel failed to approve insulin degludec (Tresiba) due to potential MACE. Ongoing CV trials being performed – look for DEVOTE data • ORIGIN – insulin glargine (2012) - retrospective • GLP cardiovascular data… • EXSCEL (2015), LEADER (2015) • Implications of lipid and HTN guidelines Lancet. 2009;373:2125-2135 BMC Endocr Disord. 2009 Jul 29;9:17 Cardiovascular Diabetology 2011, 10:22
summary • Continue to fight clinical inertia • New options for new clinical targets • Evolution of CV data for all agents • More focus on earlier diagnosis and treatment • Exciting times.
Thanks so much… Questions?