Download
1 / 56
740 likes | 1.58k Views
Idiopathic Pulmonary Fibrosis. Ganesh Raghu, MD, FACP, FCCP Professor of Medicine and Laboratory Medicine University of Washington Medical Center Chief, Chest Clinic Director: Interstitial Lung Disease and Lung Transplant Program. Classification of Idiopathic Interstitial Pneumonias.

E N D
Idiopathic Pulmonary Fibrosis Ganesh Raghu, MD, FACP, FCCP Professor of Medicine and Laboratory Medicine University of Washington Medical Center Chief, Chest Clinic Director: Interstitial Lung Disease and Lung Transplant Program
Classification of Idiopathic Interstitial Pneumonias International Consensus Statement (ATS/ ERS 2002)* *AJRCCM 105: 277-304, 2002
Classification of Idiopathic Interstitial Pneumonias International Consensus Statement (ATS/ ERS 2002)* *AJRCCM 105: 277-304, 2002
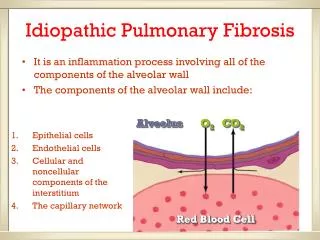
Idiopathic Pulmonary Fibrosis In spite of potent anti-inflammatory therapy: • progressive • irreversible • lethal disease
Idiopathic Pulmonary Fibrosis:Survival 100 80 60 40 20 0 % survival Treated (Prednisone alone) Untreated 0 3 6 9 12 15 18 Time (years) M. Turner-Warwick, et al. Thorax. 1980;35:593-599.
IPF and corticosteroid therapy 10-30% reported therapeutic response Problem • No biopsies • No strict definition of UIP • Includes other pathologies • Few large-scale trials
Clinical response to therapy in IPF 100 50 0 Prednisolone+cyclophosphamide Prednisolone Stable or improved (%) 1 3 12 24 36 Months Johnson MA, et al. Thorax. 1989;44:280-288.
100 80 60 40 20 0 Survival (%) 0 10 20 30 40 50 60 70 Effect of therapy of survival in IPF PrednisolonePrednisolone + Colchicine Prednisone +D-Penicillamine Prednisone + Colchicine+ D-Penicillamine Months Selman M, et al. Chest. 1998;114:507-512.
Idiopathic Pulmonary Fibrosis:Survival 100 80 60 40 20 0 Prednisone + Imuran* % Survival Treated (prednisone alone) Untreated 0 3 6 9 12 15 18 Time (years) M Turner-Warwick, et al. Thorax. 1980;35:593-599. *G. Raghu, et al. ARRD. 1991;144:291-296.
Idiopathic Pulmonary Fibrosis:Overall Survival 100 80 60 40 20 0 % survival 0 3 6 9 12 15 18 Time (years) M Turner-Warwick. Thorax. 1980;35:171.
Idiopathic Pulmonary Fibrosis (IPF)Previous and current clinical trends (Yr 2001) Disease already in mid-to-advanced stages at diagnosis Why?
Genetic predisposition ? 5 - 10 yrs 40 45 50 55 60 65 70 75 80 85 Years Years Injury Recurrent Alveolar wall 1-2 yrs Referral to centers Mild or no symptoms Middle age % Survival Years Primary MD GP Internist (Pulmonary specialist) Idiopathic Pulmonary FibrosisPrevious and current clinical pattern (Yr 2001)
Idiopathic Pulmonary Fibrosis (IPF): TreatmentChallenges and hurdles – New, multicenter, clinical trials: Yr 2001 Theoretic goals and clinical realities to improve survival Specific new Rx 100 80 60 40 20 0 • Quality of life • Minimal or no side effects • Identify complications early and Rx promptly % survival Supportive Rx Survivorship effect 5 yr 10 yr
Idiopathic Pulmonary Fibrosis (IPF): TreatmentChallenges and hurdles – New, multicenter, clinical trials: Yr 2001 Theoretic goals and realities (Yr 2001) Specific new Rx • rate of progression • Improved function • Better quality of life Functional impairment Years
Pathogenesis and course of UIP UIP Multiple microscopic foci of injury occurring over many years Focal fibroblast proliferation (fibroblastic foci) Collagen deposition Recurrent microscopic injury Progressive clinical course Death Katzenstein AL, et al. Am J Respir Crit Care Med. 1999;157:1301-1315.
Pulmonary Fibrosis of Unknown EtiologyConceptual pathogenesis of unusual interstitial pneumonia (UIP) Genetic predisposition factors Born with “normal” lung Growing ages Adult lung exposed to “fibrogenic” stimuli Environment (domestic, occupation) Drugs Cigarette smoke Autoimmune Infection (viral?) Recurrent, chronic aspiration Others ? Modulating factors Recurrent insult/injury x yrs Cell Proinflammatory Matrix Profibrotic cytokines Clinical manifestation Cell
Idiopathic Pulmonary Fibrosis • Fibroblast foci • extracellular matrix (collagens, proteoglycans) • gas exchange units Therapy – antifibrotic • fibroblast proliferation • extracellular matrix • Tissue repair (re-epithelialisation) • gas exchange units Improved outcome
New approach to IPF/UIP therapy To prevent further fibroproliferation, aka collagen production, aka scar formation
Idiopathic Pulmonary Fibrosis: Antifibrotic TherapyInterferon-g – A preliminary study Prospective study (5/96 to 2/99), open label, controlled, randomized • 18 patients, unresponsive to corticosteroids or immunosuppression during prior 12 months • 6 weeks oral prednisone (50 mg/d x 4 wks, 10 mg/d x 2 wks) • Unresponsive patients randomized - 200 mg g-IFN S/C x 3 week - plus 7.5 mg oral prednisolone vs 7.5 mg oral prednisolone alone - 12-month treatment - Follow up with PFTs Ziesche, et al. NEJM. 1999; 341:1264-1269.
Idiopathic Pulmonary Fibrosis: Antifibrotic TherapyInterferon-g – A preliminary study Conclusions • Significant improvement in PFTs in all 9 patients receiving 12 months of IFN- plus low-dose prednisolone Ziesche, et al. NEJM. 1999; 341:1264-1269.
Idiopathic Pulmonary FibrosisTreatment with Interferon-g 1b Published Study Revisited* Too good …to be true? Ziesche, et al. NEJM. 1999; 341:1264-1269. * Sponsor Intermune Pharmaceuticals, Brisbane, CA
Idiopathic Pulmonary FibrosisTreatment with Interferon-g 1b Published study revisited* Methods: Independent review of data of individual study patients • Expert panel: • Ganesh Raghu, MD (Seattle, WA) • Kevin Brown, MD (Denver, CO) • Paul Noble, MD (New Haven, CT) • Tom Colby, MD (Scottsdale, AZ) • With Rolf Ziesche, MD (Vienna, Austria) • At Mayo Clinic, Scottsdale, AZ (3/2/2000) Ziesche, et al. NEJM. 1999; 341:1264-1269. G. Raghu, et al. Independent review. March 2000 (ATS Monograph 2000.) * Sponsor Intermune Pharmaceuticals, Brisbane, CA
Idiopathic Pulmonary FibrosisTreatment with Interferon-g 1b Published study revisited/re-analyzed* Control IFN • Surgical lung bx:15/18 patients 7 8 • Transbronchial bx: 3/18 patients 2 1 • Definite IPF 5/9 4/9 • Probable IPF (UIP±NSIP/chronic HSP/other) 3/93/9 • Definitely not IPF 1/9(TBB) 2/9 Ziesche, et al. NEJM. 1999; 341:1264-1269. * G. Raghu, K. Brown, P. Noble, T. Colby: Independent Review with Rolf Ziesche:March 2000, Scottsdale, AZSponsor Intermune Pharmaceuticals, Brisbane, CA (ATS Monograph. 2000.)
Define IPF Idiopathic Pulmonary FibrosisTreatment with Interferon-g 1b Published study revisited/re-analyzed* Prednisolone alone IFN-g + low-dose prednisolone 100 100 80 80 60 60 TLC (% Predicted) TLC (% Predicted) 40 40 20 20 Probable IPF Not IPF 0 0 Baseline 12 months Baseline 12 months Ziesche, et al. NEJM. 1999; 341:1264-1269. G. Raghu, et al. Independent review. (ATS Monograph 2000.) * Sponsor Intermune Pharmaceuticals, Brisbane, CA
Define IPF Idiopathic Pulmonary FibrosisTreatment with Interferon-g 1b Published study revisited/re-analyzed* Prednisolone alone IFN-g + low-dose prednisolone 100 100 80 80 60 60 VC (%Predicted) VC (%Predicted) 40 40 20 20 Probable IPF Not IPF 0 0 Baseline 12 months Baseline 12 months Ziesche, et al. NEJM. 1999; 341:1264-1269. G. Raghu, et al. Independent review. (ATS Monograph 2000.) * Sponsor Intermune Pharmaceuticals, Brisbane, CA
Define IPF Idiopathic Pulmonary FibrosisTreatment with Interferon-g 1b Published study revisited/re-analyzed* Prednisolone alone IFN-g + low-dose prednisolone 80 80 60 60 A-a gradient A-a gradient 40 40 20 20 Probable IPF Not IPF 0 0 Baseline 12 months Baseline 12 months Ziesche, et al. NEJM. 1999; 341:1264-1269. G. Raghu, et al. Independent review. (ATS Monograph 2000.) * Sponsor Intermune Pharmaceuticals, Brisbane, CA
Idiopathic Pulmonary FibrosisTreatment with Interferon-g 1b Published study revisited* Conclusions • Patients with IPF + steroid resistant unclassifiable IIP (Not BOOP) improved with IFN-g • Some variability between Bx+HRCT findings (timing ± Bx)(sample) • Side effects: In most patients;first 3 months, intensity decreased thereafter Ziesche, et al. NEJM. 1999; 341:1264-1269. * G. Raghu, K. Brown, P. Noble, T. Colby: Independent Review with Rolf Ziesche:March 2000, Scottsdale, AZSponsor Intermune Pharmaceuticals, Brisbane, CA (ATS Monograph. 2000.)
Idiopathic Pulmonary FibrosisTreatment with Interferon-g 1b Published study revisited* Implications • Definitive phase III clinical trial with large number of well defined study patients needed to confirm the potential benefits of IFN-g in patients with IPF and IIP resistant to steroids Ziesche, et al. NEJM. 1999; 341:1264-1269. * G. Raghu, K. Brown, P. Noble, T. Colby: Independent Review with Rolf Ziesche:March 2000, Scottsdale, AZSponsor Intermune Pharmaceuticals, Brisbane, CA
Interferons and Idiopathic Pulmonary Fibrosis Summary • Type I (IFN-, , , ) and Type II (IFN-) • Distinct differences (molecular, receptor level, and inducibility) • Type I • IFN- : no role ( Bleomycin induced pulmonary fibrosis) • IFN-: Phase II, multicenter clinical trial in well defined IPF* • Not efficacious* (subgroup analyses) • Type II (IFN-) • Preliminary observation (Phase II clinical trial) promising† • Efficacy: to be determined (ongoing Phase III multicenter, clinical trial**) • Until study completed: IFN- experimental * G. Raghu et al. AJRCCM. 2001;163(5, Part 2):A707. Sponsor: Biogen Inc, Cambridge, MA † Ziesche, et al. NEJM. 1999;341:1264-1269 ** Sponsor: Intermune Pharmaceuticals, Brisbane, CA
Idiopathic Pulmonary Fibrosis (IPF): Treatment with IFN-Current status (April 2002) • Multicenter, phase III, clinical trial* (9/00 ) • Double-blind, placebo-controlled, prospective, randomized • Target N=306 (enrollment completed in US/Canada 9/01) • Current sites: US/Canada (51 sites), Europe (4), South Africa (1) • Primary endpoint • Decrease rate of progression • Minimum duration of study = 12 months (306th patient) • Randomized N=330 patients • European sites: Ireland (1), Netherlands (1), Spain (2), UK (2) • Study ongoing • Anticipated analysis: September 2002 — December 2002 * Sponsor: Intermune, Inc, Brisbane, Calif.
Idiopathic Pulmonary Fibrosis Other Potential Therapies for the Future
IFN- Other potential antifibrotic therapies for IPF Subcutaneous vs inhaled
Other potential antifibrotic therapies for IPF • N-Acetylcysteine (NAC) • Pirfenidone • Anti TGF-B therapies • Lovastatin • Relaxin • ACE Inhibitors • PGE2 • Leukotriene receptor antagonist • Endothelin receptor antagonist • Anti TNF-alpha Therapies • Others
Other potential antifibrotic therapies for IPF N-Acetylcysteine (NAC) Trial (Europe) • Glutathione deficiency in IPF (ARDS, HP) • Powerful antioxidant protecting lung epithelial cells (H2O2) • N-acetylcysteine is a GSH agonist • Extracellular glutathione suppresses human lung fibroblast proliferation • Attenuation of bleomycin model (inhaled) • Oral NAC augments lung glutathione and improves pulmonary functions in some patients with IPF • Prospective clinical trial • Prednisone + Azathioprine + NAC vsPrednisone + Azathioprine
Other potential antifibrotic therapies for IPF • Decreases fibroblast proliferation • Decreases ECM production • Inhibits TGF- collagen synthesis • Inhibitsmitogenic effects of PDGF Pirfenidone Ameliorated fibrosis in a hamster model of bleomycin lung
Other potential antifibrotic therapies for IPF Pirfenidone • Inhibits TGF- and PDGF affect on ECM production • Raghu et al. 1999 • 54 patients, open label (4.6 years mean duration) • 78% 1-year, 63% 2-year survival • Stabilization • Prospective clinical trial (Phase II, Japan) • Prednisone + Pirfenidone vsPrednisone Raghu, et al. Am J Respir Crit Care Med. 1999;159:(4):1061-1069.
Other potential antifibrotic therapies for IPF Potential anti-TGF- therapies • Antibodies • Soluble receptor • Decorin • Smad 7
Idiopathic Pulmonary Fibrosis (IPF): Yr 2002 • Well designed prospective, multicenter clinical trials • Concerted effort with dedication and commitment • Patients, physicians, investigators, health care agencies and providers, funding agencies, foundations, associations, donors, pharmaceutical companies
Idiopathic Pulmonary Fibrosis (IPF): Yr 2002Determinants of an efficacious regimen in new clinical trials • Ideal primary end point: survival • Secondary end points: change in PFTs, oxygenation (resting, exertion), imaging studies, quality of life, biological/molecular markers • Tolerance: side effects, route of administration, complications • Safety • Cost effectiveness * Personal opinion
Idiopathic Pulmonary Fibrosis (IPF): Yr 2002New, multicenter, clinical trials Environment for new directions just right ! • Emerging consensus among experts from multidisciplinary services encouraging • Several potential specific agents targeted to decrease fibrosis available • Commitment from all concerned to work in a concerted and cooperative manner • Eager physicians, investigators, patients, pharmaceutical companies • Resources becoming apparent
Idiopathic Pulmonary Fibrosis (IPF): Yr 2002New, multicenter, clinical trials Challenges and Hurdles* IPF: “Death sentence” (progressive dyspnea death within a few years of diagnosis) • Clinical/scientific factors • Behavioral patterns: physicians, patients • Health care systems • Other confounding factors * Personal observation and opinion
Idiopathic Pulmonary Fibrosis (IPF): Yr 2002 • Realistic hope for better and successful management • Awareness: distinct entity, lone corticosteroid Rx useless and harmful • Early diagnosis: better defined criteria • Referral to regional experts and centers • Initiation early Rx intervention • Careful monitoring for complications and appropriate Rx
Idiopathic Pulmonary Fibrosis (IPF): Yr 2002 • Better defined and characterized: consensus among experts • Increased awareness and cooperation: affected person/families/public; physician • Increased and earlier detection • Pathogenesis: newer concepts development of newer/better agents to abort fibrosis and enhance tissue repair • New strategies and better clinical management • Feasibility of large, multicenter, clinical trials demonstrated (-IFN trial) • Several multicenter, clinical trials ongoing worldwide:-IFN, Perfenidone, N-acetyl-cysteine, others • Hope: realistic
Idiopathic Pulmonary Fibrosis (IPF): Yr 2002New, multicenter, clinical trials A realistic hope amidst true hurdles • An evolutionary path to lessen/ease human suffering with a successful outcome is just around the corner!
ADULT LUNG TRANSPLANTATIONINDICATIONS (1983-2000) SingleLung Bilateral/Double Lung
Survival Benefit of Lung Transplantation for End-Stage Lung Disease • All patients listed for transplant with UNOS Jan 1, 1992 - Dec 31, 1994. • Included: CF (1234), IPF (919), Emphysema (2425) • Excluded: Patients supported by ventilators, children with emphysema or IPF, all patients with CF > age 50. Hosenpud, et al. Lancet 1998; 351: 24-27.
Survival while on waiting list Survival in percent Time (months) Hosenpud, et al. Lancet 1998; 351: 24-27.
Survival After Transplantation Survival in percent Time (months) Hosenpud, et al. Lancet 1998; 351: 24-27.
General Medical Conditions that Impact on Eligibility for Lung Transplantation ATS Statement AJRCCM 158: 335-339, 1998.
General Medical Conditions that Impact on Eligibility for Lung Transplantation ATS Statement AJRCCM 158: 335-339, 1998.