Download
1 / 30
1.02k likes | 5.09k Views
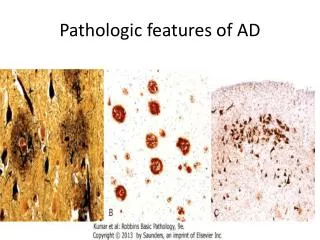
Pathologic Calcification. Doç. Dr. Işın Doğan Ekici. CALCIFICATION. Pathologic calcification is the abnormal tissue deposition of calcium salts, together with smaller amounts of iron, magnesium, and other mineral salts. It is a common process occurring in a variety of pathologic conditions.

E N D
Pathologic Calcification Doç. Dr. Işın Doğan Ekici
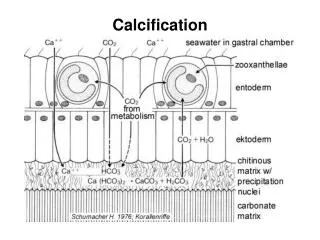
CALCIFICATION • Pathologic calcification is the abnormal tissue deposition of calcium salts, together with smaller amounts of iron, magnesium, and other mineral salts. • It is a common process occurring in a variety of pathologic conditions.
CALCIFICATION • Calcium salts(hydroxides, phosphate-hydroxides) are abnormally deposited. • Regardless of cause, calcium salts stain dark blue on H&E. • If there is any doubt, special stains like the Von Kossa of Alizarin red demonstrate it is calcium. • Pathologic calcification: • Dystrophic calcification • Metastatic calcification
Dystrophic calcification • May occur at any serum calcium level • Usually occurs in previously injured tissue • Metastatic calcification • Occurs at high serum calcium levels • Often related to bone metastases, but can occur in any organ, even in normal tissue, during periods of hypercalcemia (from whatever cause)
Dystrophic calcification • Several normal structures tend to calcify during adult life (bones, teeth, pineal gland, ect) • This is calcification that takes place locally, in the presence of normal overall calcium-phosphorus metabolism. • The calcifications may be of any size. • While a degenerated/necrotic cell whose mitochondria calcified may provide a nidus for stone-building. • In intracellular calcification, the first organelle to calcify is usually the mitochondrion.
Dystrophic calcification is encountered in areas of necrosis, whether they are of coagulative, caseous, or liquefactive type, and in foci of enzymatic necrosis of fat. • Calcification is almost inevitable in the atheromas of advanced atherosclerosis. • It also commonly develops in aging or damaged heart valves, further hampering their function
Whatever the site of deposition, the calcium salts appear macroscopically as fine, white granules or clumps, often felt as gritty deposits. • Sometimes a tuberculous lymph node is virtually converted to stone.
Examples for Dystrophic calcification: • Calcium help mammographers recognize breast cancer. • Advanced atherosclerotic plaques undergo calcification. • Malformed or damaged cardiac valves tend to calcify: • congenitally bicuspid aortic valves • aortic valve stenosis • Caseous granulomas (tuberculosis) • Scars (surgical, myocardial) • Certain tumors contain "psammoma bodies", little spherules of basement membrane that calcify • thyroid cancer, ovarian cancer, meningioma
This is dystrophic calcification in the wall of the stomach. At the far left is an artery with calcification in its wall. There are also irregular bluish-purple deposits of calcium in the submucosa. Calcium is more likely to be deposited in tissues that are damaged.
Little spherical calcifications associated with giant cells in granulomas are called "Schaumann bodies" or "conchoid bodies". • Uterine smooth muscle tumors may calcify. • Calcification of the pinna of the ear occurs for some reason in some cases of longstanding adrenocortical insufficiency (Addison's disease). • If a fetus dies and calcifies, it may be retained for years as a "lithopedion" ("stone child"). • Precipitation of calcium stearate in pancreatitis-associated fat necrosis. • Celiac plexus calcification (causes pain syndromes)
Pathogenesis of dystrophic calcification: • In the the final common pathway is the formation of crystalline calcium phosphate mineral in the form of an apatite similar to the hydroxyapatite of bone. • The process has two major phases: • initiation (or nucleation) • propagation; • both can occur intracellularly and extracellularly. • Initiation of intracellular calcification occurs in the mitochondria of dead or dying cells that accumulate calcium. • Initiators of extracellular dystrophic calcification include phospholipids found in membrane-bound vesicles about 200 nm in diameter; in cartilage and bone, they are known as matrix vesicles, and in pathologic calcification, they are derived from degenerating or aging cells.
It is thought that calcium is concentrated in these vesicles by a process of membrane-facilitated calcification, which has several steps: • (1) calcium ion binds to the phospholipids present in the vesicle membrane, • (2) phosphatases associated with the membrane generate phosphate groups, which bind to the calcium, • (3) the cycle of calcium and phosphate binding is repeated, raising the local concentrations and producing a deposit near the membrane, • (4) a structural change occurs in the arrangement of calcium and phosphate groups, generating a microcrystal, which can then propagate and perforate the membrane. • Propagation of crystal formation depends on the concentration of Ca2+ and PO4 and the presence of inhibitors and other proteins in the extracellular space, such as the connective tissue matrix proteins.
She had an ectopic pregnancy where the egg had implanted in the fallopian tube. The foetus that developed, burst out of the fallopian tube and continued to develop in the abdominal cavity. It survived by attaching it's placenta to vital organs around her stomach. Lithopedion
Metastatic calcification • It may occur in normal tissues whenever there is hypercalcemia. There are four principal causes of hypercalcemia: • (1) increased secretion of parathyroid hormone (PTH) with subsequent bone resorption, as in hyperparathyroidism due to parathyroid tumors, and ectopic secretion of PTH-related protein by malignant tumors • (2) destruction of bone tissue, occurring with primary tumors of bone marrow (e.g., multiple myeloma, leukemia) or diffuse skeletal metastasis (e.g., breast cancer), accelerated bone turnover (e.g., Paget disease), or immobilization; • (3) vitamin D-related disorders, including vitamin D intoxication, sarcoidosis (in which macrophages activate a vitamin D precursor), and idiopathic hypercalcemia of infancy (Williams syndrome), characterized by abnormal sensitivity to vitamin D; and • (4) renal failure, which causes retention of phosphate, leading to secondary hyperparathyroidism. Less common causes include aluminum intoxication, which occurs in patients on chronic renal dialysis, and milk-alkali syndrome, which is due to excessive ingestion of calcium and absorbable antacids such as milk or calcium carbonate.
Metastatic calcification may occur widely throughout the body put principally affects the interstitial tissues of the gastric mucosa, kidneys, lungs, systemic arteries, and pulmonary veins. • Although quite different in location, all of these tissues lose acid and therefore have an internal alkaline compartment that predisposes them to metastatic calcification. • In all these sites, the calcium salts morphologically resemble those described in dystrophic calcification. Thus, they may occur as noncrystalline amorphous deposits or, at other times, as hydroxyapatite crystals. • Usually, the mineral salts cause no clinical dysfunction, but, on occasion, massive involvement of the lungs produces remarkable x-ray films and respiratory deficits. Massive deposits in the kidney (nephrocalcinosis) may in time cause renal damage
Summary of Metastatic calcification: • The serum calcium and/or phosphate ion concentration is already elevated for some reason. • Healthy tissues calcify. • Causes of high blood calcium: • cancer destroying bone, • high hPTH levels (parathyroid adenomas and hyperplasias, squamous cell carcinoma of the lung, rarely others), • sarcoidosis, • vitamin D abuse, • milk and antiacid abuse.
High blood phosphate : • kidney failure • massive tumor lysis. • Metastatic calcification occurs: • in the alveolar walls, • the gastric fundic epithelium (near parietal cells), • the basement membranes of certain renal tubules, • the walls of small blood vessels. • The calcium precipitates first where there is excess hydroxyl ions.
In very severe lung or kidney involvement, respiratory insufficiency or renal tubular failure can occur. • But usually metastatic calcification is harmless evidence of serious disease elsewhere. • Calcification of collagen is diagnostic of sustained electrical injury (happens at the cathode during electrical torture). • Any kind of calcification can ossify: • produce bone and even bone marrowwith active marrow • in airway sections of elderly patients, • in calcified atherosclerotic plaques.
Here is so-called "metastatic calcification" in the lung of a patient with a very high serum calcium level (hypercalcemia).
The endocrine system contains a highly integrated and widely distributed group of organs that orchestrates a state of metabolic equilibrium, or homeostasis, between the various tissues of the body. • Signaling by extracellular secreted molecules can be classified into three types: • autocrine, • paracrine, or • endocrine, based on the distance over which the signal acts.
In endocrine signaling, the secreted molecules, which are frequently called hormones, act on target cells distant from their site of synthesis. • An endocrine hormone is frequently carried by the blood from its site of release to its target. Increased activity of the target tissue often down-regulates the activity of the gland that secretes the stimulating hormone, a process known as feedback inhibition.
Hormones can be classified into several broad categories, based on the nature of their receptors: • Hormones that trigger biochemical signals upon interacting with cell-surface receptors: This large class of compounds is composed of two groups: • (1) peptide hormones, such as growth hormone and insulin, • (2) small molecules, such as epinephrine. • Binding of these hormones to cell surface receptors leads to an increase in intracellular signaling molecules, termed second messengers, such as cyclic adenosine monophosphate (cAMP); production of mediators from membrane phospholipids (e.g., inositol 1,4,5-trisphosphate); and shifts in the intracellular levels of ionized calcium.
Several processes may disturb the normal activity of the endocrine system, including impaired synthesis or release of hormones, abnormal interactions between hormones and their target tissues, and abnormal responses of target organs to their hormones. • Endocrine diseases can be generally classified as • (1) diseases of underproduction or overproduction of hormones and their resulting biochemical and clinical consequences, • (2) diseases associated with the development of mass lesions, which may be nonfunctional or may be associated with overproduction or underproduction of hormones. • The study of endocrine diseases requires integration of morphologic findings with biochemical measurements of the levels of hormones, their regulators, and other metabolites.
In conclusion: • You will learn the pathology of endocrine system in detail next year!