Download
1 / 29
290 likes | 363 Views
Matthew Kilmurry, M.D. St. Mary’s General Hospital Grand River Hospital. Lung Cancer: A Surgeon’s Perspective. I have no conflicts of interest. The problem. 2003 numbers for Ontario 7500 new cases 6300 deaths Only 25% of cases are surgically resectable

E N D
Matthew Kilmurry, M.D. St. Mary’s General Hospital Grand River Hospital Lung Cancer: A Surgeon’sPerspective
The problem • 2003 numbers for Ontario • 7500 new cases • 6300 deaths • Only 25% of cases are surgically resectable • Breast cancer in 2007 was 8000 new cases and 2000 deaths
Causes • Smoking • Radon exposure • Asbestos exposure • Second hand smoke • Genetics
Types of Lung Cancer • Primary • Secondary • Colonic mets • Other primaries
Resection of pulmonary mets • Several prognostic factors • Disease free interval • Number of mets • Resectability • 30% long term survival • Do not assume it is a met • Old study suggests 73% of pulmonary nodules in patients with previous cancer will be new primary
Primary lung cancer • Small cell • Non small cell • Accounts for 75-80 % of primary lung tumors
Screening • No accepted screening method • Studies using CT, CXR and sputum • High index of suspicion • smokers
Staging • Stage I: no lymph node involvement • Stage II: lymph nodes involved or tumor invading into chest wall • Stage III: mediastinal nodal involvement or bad tumour factors • Stage IV: metastatic disease
Surgical Approach • Diagnosis: Is this cancer? • Metastases: Is there spread? • Suitability: Is the patient healthy enough for surgery?
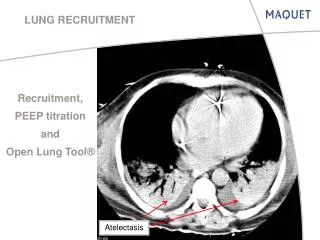
Diagnosis • History and physical • Chest X-ray • CT scan • Percutaneous biopsy • Bronchoscopy
Metastases • History and physical • Upper abdominal imaging • Bone scan and CT head • PET scan • Mediastinoscopy
Suitability • History and physical • PFT’s • Cardiac investigations • 2D echo • Stress test • Nuclear medicine • CPET • Quantitative V/Q scan
Treatment • Stage I and II are generally offered surgery with stage II getting post op chemo • Some stage III can be offered surgery – usually after chemoradiotherapy • Rare stage IV patients can be offered surgery • Solitary brain mets
Treatment • Lobectomy preferred approach • Limited resection has higher recurrence and worse long term suvival • Stage survival, 5 years • Stage I – 60-70% • Stage II – 40-50% • Stage III – 15-25% • Stage IV – 0-10%
Case # 1 • 65 year old male previous smoking history • Chest X-ray done as part of annual health exam • CT confirmed mass in LUL • Small lesion also noted in RUL
Case # 1 • Bronchoscopy and mediastinoscopy showed no evidence of mets • Thoracotomy confirmed diagnosis and had lobectomy • Right upper lobe nodule unchanged over two years
Case # 2 • 68 year old woman had pneumonia like symptoms which led to chest X-ray • Smoker of 1 pack per day for 45 years
Case # 2 • CT chest showed large tumour with no evidence of mets • Biopsy shows NSCLC • PET scan shows no evidence of metastatic disease
Case # 2 • Mediastinoscopy showed metastatic disease in lymph nodes • Referred for chemoradiotherapy • Possible candidate for surgery
Palliation • Majority of work with chemo and radiotherapy • Pain and symptom management vital • Surgery sometimes required • Pleural effusions • Endobronchial tumours
Thoracic DAU • Run through Grand River Cancer Center • Multidisciplinary clinic with respirologists and thoracic surgeons • Referrals accepted through GRCC • Main criteria is newly abnormal chest X-ray
Thoracic Program • Combined thoracic surgery at St. Mary’s General Hospital • CCO pushing to eliminate low volume thoracic centers • Working to keep thoracic surgery in Kitchener-Waterloo
Conclusions • Lung cancer is a major health concern in Ontario • Surgery offers best chance for cure in resectable cases • Multidisciplinary care required and available in our region