Download
1 / 25
260 likes | 416 Views
Amine Autacoids Histamine & 5-Hydroxytryptamine. Dr Mahmoud Khattab. Histamine Source, Storage & Release. Histamine is an amine, derived from the amino acid histidine by L-histidine decarboxylase Storage: In mast cells mainly in lungs, skin & GIT mucosa, as an inactive complex with heparin

E N D
Amine AutacoidsHistamine & 5-Hydroxytryptamine Dr Mahmoud Khattab
HistamineSource, Storage & Release • Histamine is an amine, derived from the amino acid histidine by L-histidine decarboxylase • Storage: • In mast cells mainly in lungs, skin & GIT mucosa, as an inactive complex with heparin • In platelets & basophilic leukocytes • In CNS • Enterochromaffin-like (ECL) cells of the stomach • Histamine inactivation is via N-methylation or oxidative deamination into Me-histamine/imidazole acetic acid
Histamine Release • Immunologic Release (Cell destruction): mast cell & basophils degranulate when exposed to the appropriate antigen (bacterial toxins, sing venom, cold, injury) • Chemical Release: by drugs like morphine, vancomycin & curare, X-ray contrast media, foreign proteins • Dissolution of cytoplasmic granules by radiation and surfactants
Histamine Receptors & Mechanism of Action • Histamine has four histamine H1, H2, H3, & H4 G-protein coupled receptors • Vasodilatation is via endothelial H1 receptors& smooth muscle H2 receptors • H1 stimulation → Increased intracellular Ca2+ → Activation of PLA2 → PGI2 & NO production → Diffusion to smooth muscles → vasodilatation • Contraction of bronchi, intestine & large blood vessels occur via stimulation of PLC-coupled H1 receptors followed by increased IP3 & DAG
Histamine Receptors & Mechanism of Action • Gastric acid secretion is via parietal cells H2 receptor stimulation by histamine from ECF cells • H2 receptor stimulation→ increased c.AMP → activation of H+/K+-ATPase (proton pump) • H3 receptors are located both in the CNS (histamine is a neurotransmitter) & in the periphery • Histamine on H3 receptors inhibits its own release (autoreceptors) as well as inhibition of release of other neurotransmitters (hetero-inhibitory effect) • H3 receptors appear to be coupled to Ca2 influx reduction through N-type Ca2+ channels
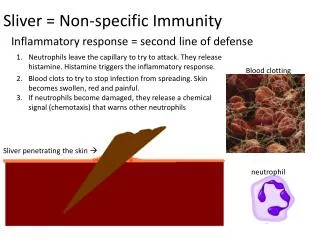
Actions of Histamine • Increased vascular permeability (H1 & H2): capillary dilation & increased permeability of post-capillary venules → leakage of plasma proteins & fluids into extracellular spaces • This leads to the dermal “triple response” upon local injury: redness, wheal formation, & flare • Heart: Increased heart rate (H2) and positive inotropic effect (H1 & H2), at moderate-high dose • Sensory nerve endings stimulation leading to pain & itching
Actions of Histamine • Stimulation of exocrine glands secretions: • Nasal & bronchial secretions (H1 receptors) • Gastric acid secretion (H2 receptors) • Stimulation of epinephrine secretion from adrenal medulla via stimulation of H1 receptors on chromaffin cells • Possible pathophysiologic role in migraine
Histamine H1 Receptor Blockers (Antihistamines) • Ethanolamines: • Diphenhydramine, Dimenhydrinate* • Ethylenediamines: • Tripelennamine, antazoline, naphazoline • Alkylamines: • Chlorpheniramine, brompheniramine • Piperazines: Cyclizine*, meclizine*, cetrizine (2ndgeneration) • Phenothiazines: Promethazine • Piperidines: (New, Second-Generation) • Loratidine, desloratidine, fexofenadine * Mainly used for prevention of nausea, vomiting & motion sickness
Antihistamines • Mechanism of Action:Competitive inhibitors for histamine at H1 receptors (structural analogs) • They antagonize all actions of histamine except for the gastric acid stimulation & H2-mediated vasodilatation • Pharmacokinetics: Well absorbed orally, max serum level in 1-2 hrs • Old first-generation agents have wide tissue distribution including CNS • Newer 2nd generation are not (non-sedative) • Duration of older members: 4-6 hrs, piperazine derivatives & 2nd generation drugs have a long duration of ≥24 hrs
AntihistaminesPharmacological Actions • Inhibition of histamine-induced contraction of respiratory & GIT smooth muscles • Abolish H1-mediated vasodilatation & increased capillary permeability • Reduction of salivary, histamine-mediated bronchial & lacrimal secretions • Most antihistamines cause CNS depression, but in some patients restlessness may occur. • The antimotion sickness effect is partly mediated through the anti-cholinergic effect
AntihistaminesReceptors Blocked & Adverse Actions • Receptors selectivity: 1st generation antihistamines are of poor H1 receptor selectivity. They block other receptors leading to adverse effects: • Cholinergic R blockade: dry mouth, urinary retention, & tachycardia • -adrenergic R blockade, by promethazine, leading to hypotension, tachycardia & dizziness • Serotonin R blockade leading to increased appetite
AntihistaminesAdverse Actions • Sedation: 1st generation antihistamines have high CNS penetration leading to sedation • In addition, they may cause tremors, dizziness, tinnitus & fatigue • 2nd generation antihistamines have no or minor sedation and other CNS effects being more specific for H1 & poor CNS penetration • This might interfere with driving ability or to work machinery (use second generation) • Anticholinergic side effects especially dry mouth & blurred vision
AntihistaminesAdverse Actions • Local anesthetic activity that can lead, at high dose level to: • CNS stimulation & convulsions, (observed in attempted suicide with antihistamines) • Cardiac depression • Drug interactions; increasing CNS sedation of other sedatives, increased activity when given with CYT P450 inhibitors (terfenadine was withdrawn) • Acute poisoning: hallucination, excitement, & convulsions (fever & flushed skin in children) • If untreated, it leads to coma & cardiorespiratory depression
AntihistaminesTherapeutic Uses • Allergic Conditions • Acute allergic rhinitis (hay fever) • Acute skin reactions (urticaria, drug rashes) • NOT in bronchial asthma or chronic skin allergies • Prevention of motion sickness & CTZ/vestibular nausea: cyclizine, meclizine & dimenhydrinate are the most effective members • OTC Sedative/hypnotics for insomnia treatment: • Diphenhydramine & doxylamine have strong sedative effect
Histamine H2 Receptor Blockers • No or little H1 receptor affinity • They block H2 receptors on gastric parietal cells attenuating gastric acid secretion • Main use is treatment of peptic ulcer • Agents include • Cimetidine • Ranitidine • Famotidine
5-Hydroxytryptamine (5-HT, Serotonin) • Serotonin is an amine synthesized from L-tryptophan by an hydroxylase enzyme • MAO & aldehyde de-hydrogenase degrade 5-HT into 5-hydroxyindoleacetic acid (5-HIAA) • Storage: • 90% is present in enterochromaffin cells of the GIT • Other in platelets & CNS
Serotonin Receptors & Functions • Seven receptors, 5-HT1- 5-HT7 for serotonin are characterized, the first four have related functions • All types are G-protein coupled receptor except 5-HT3 receptors that are inotropic receptors
Serotonin Pharmacological Actions • CNS: 5-HT plays a role in regulation of mood, food intake & sleep (5-HT1A-D) • Blood vessels: Vasodilation (5-HT1A-D) in skeletal muscles & coronaries & cerebral constriction • Vasoconstriction (5-HT2, PLC-coupled) in splanchnic, renal, pulmonary vasculature • Heart: increased heart rate & contractility (5-HT1) • Reflex cardiac slowing & hypotension via 5-HT3 receptor stimulation in coronaries & baroceptors • Stimulation of platelet aggregation
5-HT Receptor Agonists (5-HT RAs) (Triptans) • 5-HT analogues that are agonists on 5-HT1A/1D showed effectiveness against migraine • In migraine, evidence indicates the activation of the trigemino-vascular system leading to dilation & neurogenic inflammation (antidromic release of proiflammatory peptides & neuropeptides) • Mechanism: 5-HTRAs stimulate 5-HT1A/1D receptors in the intracranial vasculature & sensory nerves of the trigeminal system leading to: • Cerebral vasculature vasoconstriction • Inhibition of release of proiflammatory peptides (kinins) & neuropeptides
5-HT Receptor Agonists (5-HT RAs) (Triptans) Eletriptan, Naratriptan, Rizatriptan, Sumatriptan, Zolmitriptan • Use: Acute treatment of attacks +/-aura, not for prophylaxis • Not used in hemiplegic or opthalmogenic migraine • Not combined with ergotamine derivatives nor selective serotonin reuptake inhibitors (SSRIs) • Contraindicated with coronary artery disease, congenital heart disease, atherosclerosis, severe hypertension or seizures • Not used in patients below 18 (or <12 for Zolmitriptan) • Safety in pregnancy/lactation not tested
5-HT RAs Adverse Effects & Pharmacokinetics • Angina pectoris-like syndrome, arrhythmias, CA spasm, MI, cerebral hemorrhage, stroke & increased blood pressure in susceptible patients • Pharmacokinetics: • Mostly significant pain relief within 4 hours • Severe renal/hepatic impairment can affect their biotransformation & clearance (dose reduction) • Average oral bioavailability, sumatriptan being the lowest (14%) • Selective serotonin reuptake inhibitors (SSRIs) are used as antidepressants (Details in Depression): • Fluoxetine, paroxetine, sertaline, citalopram
Other 5-HT AntagonistsErgot Alkaloids They are of fungal origin & used as oxytocic drugs, e.g., ergometrine (ergonovine) & Me-ergometrine • Ergotamine & dihydroergotamine have 5-HT1D agonist activity, in addition to -adrenergic stimulation & direct vasoconstriction • They are used in early-onset phase of migraine • Used in combination with caffeine • Adverse effects include nausea & vasoconstriction that may lead to angina or stroke • Methysergide: discussed later slide
Peripheral 5-HT Antagonists • Methysergide: Both antagonist on 5-HT receptors & a partial agonist • Prophylactic migraine treatment • It takes 1-2 days for full effect, • Not used during acute attack • Chronic use should not exceed 6 months without 3-4 weeks methysergide-free period • Its frequent side effects limit its use; retro-peritoneal & pulmonary fibrosis, aortic/valular fibrosis, insomnia, alopecia • Dose should be gradually tapered off for2-3 weeks to avoid rebound headache
Peripheral 5-HT Antagonists • Pizotifen, a potent 5-HT & histamine antagonist used for migraine anaphylaxis reducing the frequency & severity of attacks • Side effects include drowsiness, headache, potentiation of CNS depressants, dry mouth, impotence and hepato-toxicity (chronic use) • Cyproheptadine, a potent 5-HT & histamine antagonist used as antipruritic agent • In children, it may cause weight gain & increased growth rate
Peripheral 5-HT Antagonists • Ketanserin, a 5-HT2 receptor antagonist • It causes vasodilation lowering blood pressure, and considered for hypertension treatment • It has - & H1- receptor blocking activity • Ondansetron & granisetron are 5-HT3 receptor antagonists used for prevention of nausea & vomiting caused by radiotherapy or chemotherapy • Side effects: headache, cardiac rhythm changes,