Download
1 / 168
1.68k likes | 2.85k Views
Chemotherapy-Induced Peripheral Neuropathy (CIPN): Why the complication?. By: Tiffany Marbach, RN, BSN Alverno College MSN Student Spring 2008 marbactj@alverno.edu. Navigating through this tutorial. To advance to the next slide, click on the To review the previous slide, click on the

E N D
Chemotherapy-Induced Peripheral Neuropathy (CIPN):Why the complication? By:Tiffany Marbach, RN, BSN Alverno College MSN Student Spring 2008 marbactj@alverno.edu
Navigating through this tutorial • To advance to the next slide, click on the • To review the previous slide, click on the • At any time during the tutorial you wish to review a different section of the tutorial, click on the cell at the top of the screen
Objectives At the conclusion of this tutorial, the learner should be able to: • Understand how the peripheral nervous system works, & what nerves are affected by neurotoxic agents • Describe the signs and symptoms of Chemotherapy-Induced Peripheral Neuropathy (CIPN) • Identify which types of chemotherapeutic agents contribute/cause CIPN • Understand who is more at risk for developing this complication • Describe how patients can have improved health status and outcomes when educated about how to live with CIPN, as well as how to prevent it • Understand ways to treat CIPN once it has developed
Content of Tutorial Incidence of CIPN Pathophysiology Inflammation Stress and CIPN Chemotherapy Agents Signs/Symptoms of CIPN Assessment of CIPN Patients at risk Genetics Pharmacologic Treatment Nonpharmacologic Treatment For More Information… References Patient Teaching Case Study
Incidence of CIPN • Chemotherapy is prolonging life • Cancer is becoming a chronic, manageable disease • Many nurses will encounter those affected by this common side effect • Estimated to occur in 20% to nearly 100% of cancer patients undergoing chemotherapy (Smith, Beck, & Cohen, 2008). Microsoft Image Clip Art, 2007
What is CIPN? • Characterized as injury, inflammation, or degeneration of peripheral nerve fibers • Can result in loss of motor and sensory nerve function • CIPN can result when certain chemotherapeutic agents are used to treat cancer (Marrs & Newton, 2003) • These agents can be referred to as “neurotoxic” Microsoft Image Clip Art, 2007
Why is this important for my practice? • Encountering more and more survivors with this debilitating condition • Limited research done in this area Microsoft Image Clip Art, 2007
Why is this important for my practice? Incidence increases with: • Duration of infusion (longer infusion: increased chance) • Drugs given • Previous exposure to neurotoxic drugs • Combination chemotherapies (in which more than one neurotoxic drug is given) • Co-morbidities
Rest and Review! • Why is CIPN important for all nurses to learn about? • A. It isn’t; only oncology nurses need to care about it • B. Cancer survival rates are increasing, so more nurses will have exposure to patients with this side effect • C. It is the most common chemotherapy side effect
Sorry, but that is NOT why it is important for all nurses to be educated about CIPN. Please click on the question mark below to go back and try the question again!
CONGRATULATIONS! That is exactly why all nurses should be educated on CIPN and its effects! Click on the arrow below to continue with the tutorial.
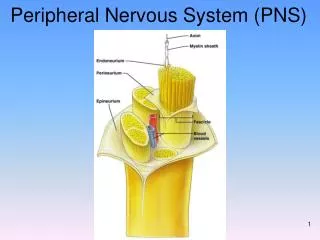
Pathophysiology of CIPN • The Peripheral Nervous System (PNS) communicates signals between the central nervous system (CNS, composed of the brain and spinal cord) and the periphery of the body(Marrs & Newton, 2003) • The peripheral nerves originate from the spinal cord • The peripheral nervous system is made of three divisions: the sensory nerves, the motor nerves, and the autonomic nerves Sheffield, Getbodysmart.com, 2008 Used with permission
Sensory nerves • Sensory nerves are responsible for detecting: • Pain • Touch • Temperature • Position • Vibration Microsoft Image Clip Art, 2007
Motor Nerves • Motor nerves are responsible for: • Voluntary movement • Muscle tone • Coordination Microsoft Image Clip Art, 2007
Autonomic nerves • Autonomic nerves are responsible for: • Intestinal motility • Blood pressure • Involuntary muscle movements Microsoft Image Clip Art, 2007
Rest and Review! • Sensory nerves are responsible for detecting: • A. Blood pressure • B. Balance and coordination • C. Intestinal Motility • D. Temperature and pain
Sorry, but that is NOT the function of the sensory nerves. Please click on the question mark below to go back and try the question again!
CONGRATULATIONS! You are correct. Sensory nerves are responsible for the feelings of temperature, pain, touch, position, and vibration. Click the arrow below to advance to the next slide.
Pathophysiology (continued) Click below for structure of neuron diagram! • Peripheral nerves are made up of individual neurons, axons, cell bodies, and dendrites, wrapped in a myelin sheath • Each nerve fiber (neuron), is made up of single axon • This axon is surrounded by Schwann cells • Schwann cells form myelin sheath • Dendrites synapse with other nerves to send a signal across from one nerve to the next (Wickham, 2007) Multiple Sclerosis Resource Centre , 2008 Used with permission
Pathophysiology (continued) • Cell body: provides nourishment and maintain the nerve fibers • Dendrites: extend from the cell body and receive/carry stimuli to the cell body • Axon: then carries the impulse away from the cell body Microsoft Image Clip Art, 2007
Pathophysiology (continued) • Peripheral nerve fibers are classified as: myelinated or unmyelinated • They are grouped to their size in diameter (called A, B, and C fibers) • A Fibers: (motor and sensory fibers), are largest in diameter, and are myelinated (allowing for fast impulse conduction)
Pathophysiology (continued) • B Fibers: (least common fiber), are smaller in diameter, and are less myelinated than A fibers • C Fibers: (some sensory and motor, but autonomic fibers are most common), smallest and slowest conducting of the PNS • Damage to the large fibers (A & B) or small fibers (C), correspond with the signs/symptoms of CIPN (Armstrong, Almadrones & Gilbert, 2005)
Sensory nerves are broken down into: Large fiber nerves: • Are myelinated • Sense position, motor control, and vibration • Composed of neurofilaments, which act as framework of axon
Sensory nerves are broken down into: Small fiber nerves: • Are unmyelinated • Include nerves that sense pain and temperature • Speed of impulse transmission depends on if neuron is highly myelinated (fast transmission), lightly myelinated (slower transmission), or unmyelinated (slowest transmission) (Wickham, 2007)
Rest and Review! • Highly myelinated nerve cells conduct impulses: • A. Fast • B. Slow • C. Very slow
Sorry! Wrong answer. Please try again. Please click on the question mark below to go back and try the question again!
Nice job!! The highly myelinated nerve cells are very fast conductors! Click the arrow below to advance to the next slide.
Rest and Review! • The function of the dendrite portion of the nerve cell is to: • A. Provide the cell with food and nourishment • B. Receive and carry stimuli to the cell body • C. Carry the impulse away from the cell body
OOPS! This is NOT the function of the dendrites… Please click on the question mark below to go back and try the question again!
Excellent answer! The dendrites are responsible for receiving and carrying stimuli to the cell body! Click the arrow below to advance to the next slide.
Pathophysiology (continued) • Peripheral neuropathy results from damage to the axon, myelin sheath, or cell body • Pathogenesis of CIPN is not completely understood • It is known that different sensations arise depending on chemotherapeutic agent administered (Wickham, 2007) Multiple Sclerosis Resource Centre , 2008 Used with permission
Pathophysiology (continued) • Chemotherapy drugs are believed to first: • Damage sensory axons • Then move on to cause degeneration and dying back of axons and myelin sheaths (Wickham, 2007) National Resource Council Canada, 2005 Used with Permission
Pathophysiology (continued) • CIPN is usually symmetrical • Begins in distal end of longest axons • Sometimes known as polyneuropathy: affects many nerves • Toxins (including chemotherapy) are transported along the axon towards the cell body (Wickham, 2007) Microsoft Image Clip Art, 2007
The stocking/glove phenomena: Moves distal to proximal • CIPN usually progresses from toes to feet to ankles to lower legs (stocking distribution) • Upper extremity damage usually comes later • Moves from fingertips to fingers to hands (glove distribution) (Wickham, 2007) Microsoft Image Clip Art, 2007
Rest and Review! • Nerve cells are damaged by chemotherapy because: • A. They aren’t strong enough to handle the toxicity • B. The chemotherapy causes degeneration and dying back of axons and myelin sheaths • C. The chemotherapy doesn’t affect the nerve cells
No…That’s not how nerve cells are damaged… Please click on the question mark below to go back and try the question again!
You’re RIGHT! That is exactly how nerve cells are damaged! Click the arrow below to advance to the next slide.
Rest and Review! • In a typical pattern of CIPN, the person experiences neuropathy first in the: • A. Upper leg • B. Toes • C. Hands • D. Upper arm
Think again. Where does neuropathy usually show up first in a stocking-glove pattern? Please click on the question mark below to go back and try the question again!
GREAT job! The neuropathies usually show up first in the lower extremities, and progress later towards the upper extremities. Click the arrow below to advance to the next slide.
Nerve Growth Factor • Axons regenerate if toxic agent removed • Damage to cell bodies is not completely reversible • Nerve Growth Factor (NGF) plays role in neuron repair • NGF is usually reduced after neurotoxic chemotherapy • Animal studies show if given NGF, some neuropathy and neural structural changes were prevented or reversed • Exact mechanism not well understood (Wickham, 2007) Microsoft Image Clip Art, 2007
Inflammation and CIPN: What’s the connection? • Tissue repair is part of the inflammatory process • It is an attempt to maintain normal body structure and function • Cell regeneration can vary depending on tissue/cell type • Three types of cells that are divided according to ability to undergo regeneration: labile, stable, or permanent cells(Porth, 2005) Microsoft Image Clip Art, 2007
Nerve cells: Permanent/Fixed Cells • Labile cells: regenerate and divide throughout life (ex: Epithelial cells found on skin or in the mouth) • Stable Cells: stop dividing when growth ends, but can regenerate when confronted with certain stimuli (ex: liver cells) • Permanent/Fixed cells: cannot undergo mitotic division, and can’t regenerate (ex: nerve and cardiac muscle cells) (Porth, 2005) Microsoft Image Clip Art, 2007
Nerve cells: Permanent/Fixed Cells (continued) • When nerve cell is damaged (for example, from a chemotherapy drug), it can not be replaced • It is replaced with scar tissue • This scar tissue can not function like the destroyed cell can (for example, can’t conduct impulses) (Porth, 2005) Microsoft Image Clip Art, 2007
Rest and Review! • Peripheral nerve cells are considered: • A. Labile cells • B. Stable cells • C. Permanent or fixed cells
This is not what nerve cells are classified as… Please click on the question mark below to go back and try the question again!
Right on! Nerve cells are fixed or permanent cells, that can not regenerate! Click the arrow below to advance to the next slide.
Stress and CIPN: What’s the connection? • CIPN can often lead to pain symptoms • This pain is classified as acute or chronic pain • Acute pain: lasts less than 6 months • Chronic pain: lasts 6 months or longer (Porth, 2005) Microsoft Image Clip Art, 2007
Stress and CIPN: What’s the connection? (continued) • CIPN can be considered acute or chronic • This depends on length of treatment, co-morbidities (pre-existing conditions beside the CIPN), and disease state • This can cause physiologic, psychological, familial, and economic stress • Chronic pain can lead to loss of appetite, sleep disturbance, and depression(Porth, 2005) Microsoft Image Clip Art, 2007
Stress and CIPN: What’s the connection? (continued) Two factors determine nature of stress: • 1. Properties of the stressor • 2. The condition of the person under stress • Severe, prolonged physical and psychological distress disrupts health with chronic stress (Porth, 2005) Microsoft Image Clip Art, 2007