Download

1 / 24
290 likes | 461 Views
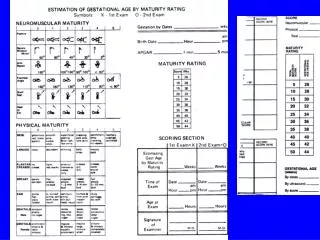
Small for gestational age (SGA) or IUGR. Definition;. SGA or IUGR is considered when the weight of baby is below the 5th percentile of growth for gestational age.

E N D
Definition; SGA or IUGR is considered when the weight of baby is below the 5th percentile of growth for gestational age. IUGR is present when fetal growth stops and, with time, falls below the 5th percentile of growth for gestational age or when growth proceeds slowly but the absolute size remains less than the 5th percentile.
Causes: I. Fetal causes: 1. Chromosomal abnormalities (Trisomies). 2. Chronic fetal infections (syphilis, rubella). 3. Congenital abnormalities. 4. Radiation. 5. Multiple gestation.
II. Placental causes: 1. Placental tumors. 2. Placental separation. 3. Twin-twin transfusion syndrome. 4. Placental infarction.
III. Maternal causes: 1. Toxemia of pregnancy. 2. Hypertension, renal diseases, or both. 3. Malnutrition or chronic illnesses. 4. Hypoxemia (due to heart or pulmonary diseases, or high altitude). 5. Sickle cell disease. 6. Smoking, alcohol consumption, and usage of anti-metabolite drugs. 7. Short stature.
Clinical features: 1. Thin, long baby. 2. Wrinkled dry skin. 3. Old man face appearance due to little subcutaneous fat. 4. Large head with small body. 5. Very alert baby (wide awake expression). 6. Transverse cracks in chest and abdomen. 7. Meconium staining of skin, umbilical cord and nails.
Problems (complications) of IUGR or SGA and their pathogenesis:
Problems (complications) of IUGR or SGA and their pathogenesis:
Problems (complications) of IUGR or SGA and their pathogenesis:
Management of IUGR: Its directed to the complications of IUGR especially perinatal asphyxia, polycythemia, hypoglycemia, and hypothermia in addition to the nutritional support.
Outcome (prognosis) of IUGR or SGA Its depend on the cause of IUGR and associated complications after birth. Fetuses subjected to chronic intrauterine hypoxia as a result of uteroplacental insufficiency are at an increased risk of birth asphyxia, polycythemia and hypoglycemia. Fetuses with IUGR resulting from chromosomal or multiple congenital anomaly syndromes have poor outcomes depend on the prognosis of these syndromes.
Fetuses born to small mothers or fetuses with poor nutritional intake usually do well and may catch-up growth after birth.
Large for gestational age Is birth weight above the 90th centile or 2 standard deviations above the mean body weight for gestational age (> 4000 g). These infants are usually born at term, but they might be preterm with weight high for gestational age.
Clinical features: 1. Macrosomia. 2. Cushinoid face. 3. Plethoric (deep red skin). 4. Thick dark hair and thick skin.
Predisposing factors: 1. Maternal diabetes mellitus. 2. Maternal obesity. 3. Old age mothers. Complications; 1. Increased incidence of birth injuries especially cervical and brachial plexus injuries, fractures clavicle, subdural hemorrhage, phrenic nerve injury with diaphragmatic paralysis, and ecchymosis of face and head.
2. Intellectual and mental retardations. 3. Congenital anomalies (especially of the heart). 4. Severe hypoglycemia due to exposure to high level of glucose in utero which causes hyperplasia of islets cells of pancrease leading to hyperinsulinism. 5. Hyperbilirubinemia.
Management: 1. Check blood glucose levels and start feeding or I.V. glucose as early as possible to avoid hypoglycemia and treat hypoglycemia when present. 2. Check serum calcium and treat hypocalcaemia when present. 3. Detect any congenital anomalies. 4. Treat jaundice. 5. Careful examination for birth injuries.
Post-term infants "postmaturity" Definition: Post-term infants are those born after 42 wk of gestation regardless of birth wt. Causes are unknown.
Clinical features: 1. Increased birth weight. 2. Absence of lanugo hair. 3. Decreased or absent vernix caseosa. 4. Long nails, abundant scalp hair, with white desquamating skin. 5. Increased alertness. 6. Meconium stained skin, umbilical cord and amniotic fluid.
Treatment: 1. Careful obstetric monitoring. 2. Induction of labor or cesarean section indicated in old primigravidas who go more than 2-4 wk beyond term. 3. Symptomatic treatment for meconium aspiration pneumonia or HIE Prognosis: Significant increase in the mrtality rate (3 times more than term infants) if delivery doelayed 3 wk or more beyond term. Thank you for your attention