Download
1 / 13
130 likes | 340 Views
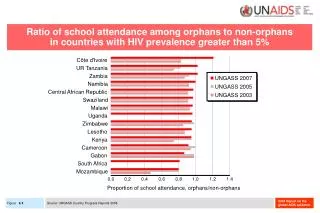
Do orphans report worse caregiver interactions and psychological and health-related outcomes than non-orphans in mixed households?. Candice Reardon, Gavin George, Kaymarlin Govender & Tim Quinlan Health Economics and HIV and AIDS Research Division

E N D
Do orphans report worse caregiver interactions and psychological and health-related outcomes than non-orphans in mixed households? Candice Reardon, Gavin George, Kaymarlin Govender & Tim Quinlan Health Economics and HIV and AIDS Research Division University of KwaZulu-Natal, South Africa 20th International AIDS Conference, Melbourne, Australia, July 2014
In collaboration with Center for International Health & Development, Boston University School of Public Health
Background The majority of children in South Africa do not live in dual parent households. The 2013 SA Child Gauge reported that only 33% of children live with both parents, 4% with their father only and 39% with their mother only (Meintjes & Hall, 2013). Studies have shown significant negative association between AIDS orphaning and children’s mental, physical and behavioural health, such as social delinquency, concentration difficulties, food insecurity, relative lack of positive peer attachments and low expectations of personal future. However, the research literature also shows that AIDS orphaning is not a definitive, determinant factor affecting the welfare of the children: there is considerable variation in the results of studies, including no significant relationships, amongst the body of South African research.
Study foci Our foci are the psychosocial welfare of orphans and non-orphans living in mixed households, measured according to anxiety/depression, affability and resilience indices, and the affective relationship between the children and their caregivers, assessed in terms of children’s communication with caregivers about personal problems.
Methodology Study site The study was conducted in Amajuba District of the KwaZulu-Natal province in South Africa. The population of the district are challenged by high levels of poverty, with both urban and rural areas experiencing high levels of unemployment due to the decline in the coal industry (Amajuba District Municipality, 2010). HIV and AIDS prevalence in the Amajuba district has fallen from 46% in 2006 (15 to 49 year old pregnant women being tested positive for HIV in antenatal clinics) to 37.3% in 2009 (Department of Health, 2009). The study population consisted of Zulu and English speaking school-going children (aged 9-15 years) and their caregivers and/or heads of household.
Methodology Analysis Descriptive statistics (means, standard deviations and frequencies) were used to assess the sample characteristics, including the age and gender of the child, orphan type, size of the mixed households, monthly income per capita and gender of the caregiver. Means, standard deviations and frequencies were conducted to evaluate participants’ overall scores for anxiety/depression, affability, resilience, caregiver interaction variables and substance use and sexual practices. Bivariate analyses (Chi square tests and independent samples t-tests) were conducted in order to examine whether any of the sample characteristics varied between orphans and non-orphans in mixed households. Correlations, chi square tests and ANOVAs were used to identify any important covariates of the outcomes of interest to determine whether these had to be controlled for in further analyses.
Results Anxiety/depression, affability and resilience showed no significant associations with any variables that were considered potentially important covariates such as household size, monthly income per capita, child age and gender, caregiver gender and caregiver relationship to child. Overall, child participants reported frequent communication with caregivers about their problems, with over half (54.3%, n = 70) reporting they ‘always’ spoke to their caregiver. The reported frequency of caregiver help and assistance was even higher, with just under two thirds (63.6%, n = 82) agreeing their caregiver ‘always’ provides help and assistance to them.
Results cont. Note: Missing cases not included • Psychosocial outcomes and caregiver-child interaction variables among orphans and non-orphans in mixed households (n = 134)
Results cont… The prevalence of substance use and sexual activity was low among the child participants. Only a handful reported ever having had smoked (9.8%, n = 13), drunk alcohol (4.5%, n = 6), used drugs (2.3%, n = 3) and had sex (5.3%, n = 7). The odds of having used cigarettes or engaged in sexual activity did not differ significantly between orphans and non-orphans in the sample.
Results cont… Substance use and sexual practices among orphans and non-orphans in mixed households (n = 134) ∞Final model including child age, child gender and ever used cigarettes, Χ2(3) = 11.07, p = .01 □ Final model including child age and ever had sex, Χ2(2) = 8.21, p<.05
Discussion Overall, the analysis found that orphans in mixed households did not report worse psychosocial outcomes (anxiety/depression, affability and resilience) than non-orphans in similar type households. Engagement in risk activities did not differ between orphans and non-orphans, contrary to what other studies have found, suggesting perhaps that environmental factors and caregiving arrangements, which were relatively similar between orphans and non-orphans in this sample, may play a greater role in risk activities than orphan status alone. Our findings throws caution to social protection responses that are financial or material in nature and targeted specifically towards orphans, or AIDS orphans in particular, given that both orphans and non-orphans from mixed households were relatively as ‘poor’ as one another.
Conclusion The findings indicate that orphans in mixed households were no worse off in terms of anxiety/depression, affability and resilience in comparison to non-orphans in similar type households. The findings call for greater thoughtfulness in how we define orphanhood, as even children with living parents had other relatives identified as their primary caregivers. Caution is emphasised with regards to decisions being made about which children are considered most vulnerable in contexts of poverty and high HIV prevalence, and to whom responses should be targeted, whether this be to orphans only or mixed households as a whole.
We thank the participants of the study for their cooperation and the ACHWRP team for their invaluable input and support. This project was funded by the National Institute of Child Health and Development (NICHD) of the United States National Institutes of Health (NIH) under its African Partnerships program (Grant R29 HD43629). Acknowledgments