Download
1 / 69
690 likes | 810 Views
Influenza, Risk Reduction and Vaccine Shortage: An Update. Marguerite A. Neill, MD Ocean State Ethics Network December 2, 2004. Why are we here?. Influenza: the Disease. Acquired by inhalation of droplet nuclei; highly contagious

E N D
Influenza, Risk Reduction and Vaccine Shortage: An Update Marguerite A. Neill, MD Ocean State Ethics Network December 2, 2004
Influenza: the Disease • Acquired by inhalation of droplet nuclei; highly contagious • Causes destruction of ciliated epithelium → risk for secondary bacterial pneumonia (pneumococcus, Staph aureus) • Can cause primary pneumonia • Severe disease in elderly, pregnant women, immunocompromised • Complications: myocarditis, rhabdomyolysis
http://www.cdc.gov/flu/weekly/weeklyarchives2003-2004/03-04summary.htmhttp://www.cdc.gov/flu/weekly/weeklyarchives2003-2004/03-04summary.htm
Influenza: The Battle Plan • Prevention • Vaccination • Diagnostics • Infection Control • Prevention of transmission • Rx and PEP
Influenza Program Plans Before October 5, 2004 • Season’s assets • Aggressive ACIP recommendations • Record number of doses • Enhanced interest in influenza • Season’s challenges • Using all doses produced • Fulfilling VFC entitlement • Coverage disparities
Influenza Vaccine 2004-2005 • The UK Medicines and Healthcare Products Regulatory Agency (MHRA) has suspended Chiron’s license to manufacture Fluvirin® vaccine in its Liverpool facility for 3 months, preventing any release of the vaccine for this influenza season • On October 5, 2004, Chiron informed CDC that none of its influenza vaccine (~48 million doses) would be available for distribution this season
Expected Pattern of TIV Distribution On October 5 • Gap in distribution for customers who pre-booked orders with Chiron • Large scale geographic disparities unlikely since both companies served all regions • Extreme dichotomization of distribution most pronounced at local level
Immediate Steps Taken • Aventis Pasteur (AvP) halted shipment of their remaining 22 M doses • ACIP met in emergency session to reduce the targeted groups • 185 M overall 98 M • 20 M children 9 M children • CDC and AvP began formulating an allocation plan for remaining inactivated influenza vaccine
Who Should NOT Receive Influenza Vaccine This Year • Healthy persons 2-64 years of age • Household contacts of high-risk persons EXCEPT children <6 months of age • Providers of essential community services* • Foreign travelers* • Students* *except those who are in a priority group because of age or medical condition
Public Health Challenge • Allocate 22 M doses as well as possible to fill the critical distribution gaps • Facilitate community efforts • Redistribute vaccine • Identify providers for targeted individuals • Reduce inappropriate vaccination • Make effective use of LAIV • Identify any other sources of vaccine
Influenza Vaccine AllocationGoal and Approach • Goal: Distribute a scarce resource to the providers most likely to be able to reach priority patients. • Two-phased approach • National level efforts to allocate vaccine quickly to providers serving priority groups (Phase I) • State and local public health efforts to guide allocation efforts later in the vaccination season based on information about unfilled orders, local supply, and number of priority persons (Phase II)
Two-phased Approach • Phase I: Orders that were immediately identifiable on October 5, 2004 • Phase II: Orders that required identification and enumeration • Separation into two phases allowed resumption of shipping to begin reaching ACIP priority groups as quickly as possible
Phase II Allocation Formula (I) • Total number priority persons in a state: estimated by census data, prevalence estimates for medical conditions • Number of doses already delivered to the state through phase 1, subtracted from the total number of doses needed for all priority persons = state’s estimated unmet need. • Add all estimates of states’ unmet needs to estimate national unmet need. • A state’s allotment of doses will be determined by dividing that state’s unmet need estimate by the national unmet need estimate, then applying the percentage to 7.2 million doses
Phase II Allocation Formula (II) • Example: • State A has 100,000 priority persons • Has received 50,000 doses to date, then • Unmet need = 50,000 doses • If the national unmet need is 50,000,000 doses, then 50,000/50,000,000 = 0.001. • State A’s unmet need represents 0.1% of the national unmet need. State A would thus be allocated 7,200 doses (0.001 x 7,200,000).
Challenges for Influenza Vaccination at the Local Level • Vaccination is later than desirable • Not enough vaccine for the current priority groups • How to mobilize clinical sector care for rapid vaccination: • Identify candidate vaccinees from the population served • Notify the patients • Actually deliver vaccine
Local Considerations in Allocating Influenza Vaccine • Identify the purpose of vaccination: • Prevent complications or death • Prevent transmission • Articulate the rationale for the decisions • Be transparent • Acknowledge the importance of speed in decision-making and implementation of vaccination.
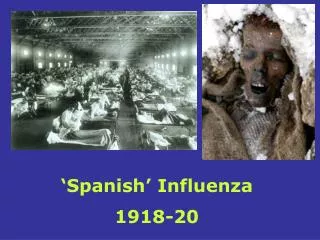
1918 Influenza Epidemic:Emergency hospital, Camp Funston, Kansas National Museum of Health and Medicine, Armed Forces Institute of Pathology, Washington, D.C.,
Avian influenza • Summer 2004 – new outbreaks in Asia; 5 dead in Vietnam & Thailand • Winter 2003/2004 - unprecedented outbreak of H5N1 in Asia; 23 deaths; mortality rate 30-60% • H7 virus found in poultry in US • 2 cases of H7 virus in Canada • Bird hosts carry virus in saliva, nasal secretions, and feces; human cases via close contact • Will poultry to human transmission presage human to human transmission?
WHO Executive Summary on Pandemic Influenza (9/14/04) “Never before has an avian influenza virus with documented ability to infect humans caused such widespread outbreaks in birds in so many countries. This unprecedented situation has significantly increased the risk for the emergence of an influenza pandemic.”
Influenza Virus • RNA virus, 2 major types cause disease in humans (A and B) • Antigenic drift: point mutations → slight variations in surface proteins • Antigenic shift: genetic reassortment of genes from different strains, some from animal reservoirs
Priority Groups For Influenza Vaccination, 2004-2005 • Children 6-23 months of age • Adults >65 years • Persons 2-64 years of age with underlying chronic medical conditions • Women who will be pregnant during influenza season MMWR 2004;53(39);923-4
Inactivated Influenza VaccineRecommendations • Persons with the following chronic illnesses should be considered for inactivated influenza vaccine: • pulmonary (e.g., asthma, COPD) • cardiovascular (e.g., CHF) • metabolic (e.g., diabetes) • renal dysfunction • hemoglobinopathy • immunosuppression, including HIV infection MMWR 2004;53 (RR-6);1-40
Priority Groups For Influenza Vaccination, 2004-2005 • Residents of nursing homes and long-term care facilities • Children 6 months-18 years of age on chronic aspirin therapy • Healthcare workers with direct, face-to-face patient contact • Household contacts and out-of-home caregivers of children aged <6 months MMWR 2004;53(39);923-4
Prevention and Control of Influenza in Healthcare Facilities • The most important measure to protect patients from influenza in a healthcare setting is vaccination of both patients and healthcare workers • In a vaccine shortage situation vaccination of HCWs becomes even more critical
Influenza Vaccination of Healthcare Workers • Reduces influenza-related death among nursing home residents • Reduces overall illness in nursing home residents • Reduces illness and illness-related absenteeism Reference: Improving Influenza Vaccination Rates in Healthcare Workers. Strategies to Increase Protection for Workers and Patients. Available at www.nfid.org
Influenza Vaccination of Healthcare Workers • Only 38 percent of U.S. healthcare workers were vaccinated in 2002
MHRI, 2003-2004Influenza Vaccination (Not including VFC)
Live Attenuated Influenza Vaccine • FluMist®, produced by MedImmune • Produced by reassortant gene technology • Viruses express contemporary influenza vaccine antigens • Administered by nasal spray
Live Attenuated Influenza VaccineIndications • Healthy* persons 5–49 years of age • Household contacts of persons at increased risk of complications of influenza; for 2004-05, just those <6 months of age • Health care workers *Persons who do not have medical conditions that increase their risk of complications of influenza
Live Attenuated Influenza VaccinePersons Who Should NOT Be Vaccinated • Children <5 years of age* • Persons >50 years of age* • Persons with underlying medical conditions* • asthma, reactive airways disease or other chronic pulmonary condition • cardiovascular disease • metabolic diseases (e.g. diabetes) • renal disease • hemoglobinopathy (e.g. sickle cell disease) *These persons should receive inactivated influenza vaccine
Live Attenuated Influenza VaccinePersons Who Should NOT Be Vaccinated • Pregnant women* • Persons immunosuppressed from disease (including HIV) or drugs* • Children or adolescents receiving long-term therapy with aspirin or other salicylates* • Severe (anaphylactic) allergy to egg or other vaccine components • History of Guillain-Barre´ syndrome *These persons should receive inactivated influenza vaccine
Live Attenuated Influenza VaccineTransmission of Vaccine Virus • Vaccinated children shed vaccine viruses for up to 3 weeks (mean, 7.6 days) • One documented instance of transmission of vaccine virus to a contact (in a daycare setting) • Transmitted virus remained attenuated • Frequency of shedding among adults : Limited (50%) early shedding up to 3 days after vaccination with very low viral titer
Use of LAIV Among Healthcare Personnel • No data regarding transmission from adults vaccinated with LAIV to immunosuppressed persons (but no evidence of transmission during 2003-2004 influenza season) • ACIP recommends that LAIV can be given to eligible HCWs except those who may expose severely immuno-suppressed persons
Use of LAIV Among CloseContacts of High-Risk Persons • Persons who receive LAIV should refrain from contact with severely immunosuppressed persons for 7 days after vaccination • Persons who receive LAIV need NOT be excluded from visitation of patients who are not severely immunosuppressed MMWR 2004;53(RR-6);17
Administration of LAIV • Severely immunosuppressed persons should not administer LAIV • Other persons at high risk for influenza complications may administer LAIV • Gloves and masks are not required
Influenza Diagnostics • Viral culture of respiratory tract specimen • Rapid tests: variable sensitivity and specificity (A vs A and B) • More useful epidemiologically than clinically • RT-PCR • Serology
Influenza A Rapid Tests: Per cent Positivity / WeekDecember, 2003
Infection Control and Prevention of Influenza Transmission • Avoid close contact with people who are sick • Stay home when you are sick • Cover Your Cough • Frequent handwashing • Avoid touching eyes, nose or mouth • Antiviral drugs
Influenza Rx and Prophylaxis • Rx only effective if started within 36 hrs of symptom onset; decreases duration of symptoms and viral shedding • For Rx, recommended to use NAI (oseltamivir and zanamivir) – limited supplies • For chemoprophylaxis, suggest using adamantines (amantidine, ramantidine)
Influenza Vaccine DistributionUnited States, 2004 • Aventis Pasteur (AvP) collaboration with CDC • Includes 22.4 million unshipped doses of 55.4 million total AvP production • Phase I of this distribution = 14.2 million doses • About 2 million doses of FluMist® to be available