Download
1 / 1
10 likes | 163 Views
History of Peripartum Cardiomyopathy and Current Pregnancy Outcome Eliza M.N (1), Quek Y.S. (1), Woon S.Y. (1), Ravichandan N. (2), Ravichandran J. (1) 1. Hospital Sultanah Aminah Johor Bahru, Malaysia 2. Singapore General Hospital. OPTIONAL LOGO HERE. OPTIONAL LOGO HERE. Objectives.

E N D
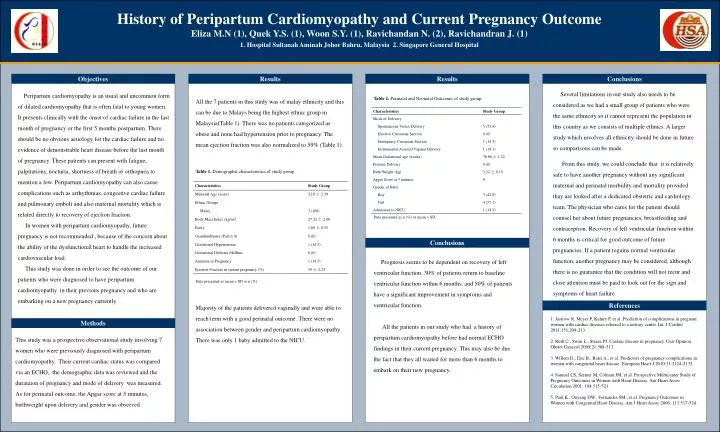
History of Peripartum Cardiomyopathy and Current Pregnancy Outcome Eliza M.N (1), Quek Y.S. (1), Woon S.Y. (1), Ravichandan N. (2), Ravichandran J. (1) 1. Hospital Sultanah Aminah Johor Bahru, Malaysia 2. Singapore General Hospital OPTIONALLOGO HERE OPTIONALLOGO HERE Objectives Results Results Conclusions Several limitations in our study also needs to be considered as we had a small group of patients who were the same ethnicity so it cannot represent the population in this country as we consists of multiple ethnics. A larger study which involves all ethnicity should be done in future so comparisons can be made. From this study, we could conclude that it is relatively safe to have another pregnancy without any significant maternal and perinatal morbidity and mortality provided thay are looked after a dedicated obstetric and cardiology team. The physician who cares for the patient should counsel her about future pregnancies, breastfeeding and contraception. Recovery of left ventricular function within 6 months is critical for good outcome of future pregnancies. If a patient regains normal ventricular function, another pregnancy may be considered, although there is no guarantee that the condition will not recur and close attention must be paid to look out for the sign and symptoms of heart failure. Peripartum cardiomyopathy is an usual and uncommon form of dilated cardiomyopathy that is often fatal to young women. It presents clinically with the onset of cardiac failure in the last month of pregnancy or the first 5 months postpartum. There should be no obvious aetiology for the cardiac failure and no evidence of demonstrable heart disease before the last month of pregnancy. These patients can present with fatigue, palpitations, nocturia, shortness of breath or orthopnea to mention a few. Peripartum cardiomyopathy can also cause complications such as arrhythmias, congestive cardiac failure and pulmonary emboli and also maternal mortality which is related directly to recovery of ejection fraction. In women with peripartum cardiomyopathy, future pregnancy is not recommended , because of the concern about the ability of the dysfunctional heart to handle the increased cardiovascular load. This study was done in order to see the outcome of our patients who were diagnosed to have peripartum cardiomyopathy in their previous pregnancy and who are embarking on a new pregnancy currently All the 7 patients in this study was of malay ethnicity and this can be due to Malays being the highest ethnic group in Malaysia(Table 1). There was no patients categorized as obese and none had hypertension prior to pregnancy. The mean ejection fraction was also normalized to 59% (Table 1). Table 2. Perinatal and Neonatal Outcomes of study group Table 1. Demographic characteristics of study group Data presented as n (%) or mean ± SD. Conclusions Prognosis seems to be dependent on recovery of left ventricular function. 30% of patients return to baseline ventricular function within 6 months, and 50% of patients have a significant improvement in symptoms and ventricular function. All the patients in our study who had a history of peripartum cardiomyopathy before had normal ECHO findings in their current pregnancy. This may also be due the fact that they all waited for more than 6 months to embark on their new pregnancy. Data presented as mean ± SD or n (%). Majority of the patients delivered vaginally and were able to reach term with a good perinatal outcome. There were no association between gender and peripartum cardiomyopathy. There was only 1 baby admitted to the NICU. References 1. Jastrow N, Meyer P, Kahiry P, et al. Prediction of complications in pregnant women with cardiac diseases referred to a tertiary center. Int. J Cardiol 2011;151:209-213. 2. Ruth C., Swan L., Steera PJ. Cardiac disease in pregnancy. Curr Opinion Obstet Gynecol 2009;21:508-513. 3. Willem D., Eric B., Balci A., et al. Predictors of pregnancy complications in women with congenital heart disease. European Heart J 2010;31:2124-2132. 4. Samuel CS, Sermer M, Colman JM, et al. Prospective Multicenter Study of Pregnancy Outcomes in Women with Heart Disease. Am Heart Assoc Circulation 2001; 104:515-521. 5. Paul K., Ouyang DW., Fernandes SM., et al. Pregnancy Outcomes in Women with Congenital Heart Disease. Am J Heart Assoc 2006; 113:517-524. Methods This study was a prospective observational study involving 7 women who were previously diagnosed with peripartum cardiomyopathy. Their current cardiac status was compared via an ECHO, the demographic data was reviewed and the durataion of pregnancy and mode of delivery was measured. As for perinatal outcome, the Apgar score at 5 minutes, birthweight upon delivery and gender was observed.