Download
1 / 41
410 likes | 420 Views
Chapter 6: Bones and Skeletal Tissues. Epiglottis. Larynx. Cartilage in external ear. Cartilages in nose. Thyroid cartilage. Trachea. Articular Cartilage of a joint. Cricoid cartilage. Lung. Cartilage in Intervertebral disc. Costal cartilage. Respiratory tube cartilages

E N D
Epiglottis Larynx Cartilage in external ear Cartilages in nose Thyroid cartilage Trachea Articular Cartilage of a joint Cricoid cartilage Lung Cartilage in Intervertebraldisc Costal cartilage Respiratory tube cartilages in neck and thorax Pubic symphysis Bones of skeleton Axial skeleton Meniscus (padlike cartilage in knee joint) Appendicular skeleton Cartilages Articular cartilage of a joint Hyaline cartilages Elastic cartilages Fibrocartilages
Skeletal Cartilages • Contain no blood vessels or nerves • Dense connective tissue girdle of perichondrium contains blood vessels for nutrient delivery to cartilage • 3 types: • Hyaline cartilages • Provide support, flexibility, and resilience • Most abundant type • Elastic cartilages • Similar to hyaline cartilages, but contain elastic fibers • Fibrocartilages • Collagen fibers—have great tensile strength
Growth of Cartilage • Appositional • Cells secrete matrix against the external face of existing cartilage • Interstitial • Chondrocytes divide and secrete new matrix, expanding cartilage from within • Calcification of cartilage occurs during • Normal bone growth • Old age
Bones of the Skeleton • Two main groups, by location • Axial skeleton: long axis of body: skull, vertebral column, rib cage • Appendicular skeleton: upper and lower limbs that attach to axial skeleton
Types of bones Long bones: longer than wide Flat bones: thin, flat, slightly curved Short bones • Cube shaped bones (in wrist and ankle) • Sesamoid bones (within tendons, e.g., patella) Irregular bones: complicated shapes
Functions of Bones • Support for the body and soft organs • Protection for brain, spinal cord, and vital organs • Movement: Levers for muscle action • Storage of minerals (calcium and phosphorus) • Storage of growth factors (like insulin-like growth factor) in bone matrix • Blood cell formation (hematopoiesis) in marrow cavities • Triglyceride (energy) storage in bone cavities
Bone Markings • Bulges, depressions, and holes serve as • Sites of attachment for muscles, ligaments, and tendons • Joint surfaces • Conduits for blood vessels and nerves
Bone Markings: Projections • Sites of muscle and ligament attachment • Tuberosity—rounded projection • Crest—narrow, prominent ridge • Trochanter—large, blunt, irregular surface • Line—narrow ridge of bone • Tubercle—small rounded projection • Epicondyle—raised area above a condyle • Spine—sharp, slender projection • Process—any bony prominence
Bone Markings • Projections that help to form joints • Head: bony expansion carried on a narrow neck • Facet: Smooth, nearly flat articular surface • Condyle: Rounded articular projection • Ramus: Armlike bar
Bone Markings: Depressions and Openings • Meatus: Canal-like passageway • Sinus: Cavity within a bone • Fossa: Shallow, basinlike depression • Notch: indentation at the edge of a structure • Groove: Furrow • Fissure: Narrow, slitlike opening • Foramen: Round or oval opening through a bone
Bone Textures Compact bone Spongy bone • Compact bone • Dense outer layer • Spongy (cancellous) bone • Honeycomb of trabeculae
Structure of a Long Bone • Diaphysis (shaft) • Compact bone collar surrounds medullary (marrow) cavity • Medullary cavity in adults contains fat (yellow marrow) • Epiphyses • Expanded ends • Spongy bone interior • Epiphyseal line (remnant of growth plate) • Articular (hyaline) cartilage on joint surfaces
Articular cartilage Proximal epiphysis Compact bone Spongy bone Epiphyseal line Compact bone Medullary cavity Diaphysis Distal epiphysis
Membranes of Bone • Periosteum • Outer fibrous layer • Inner osteogenic layer • Osteoblasts (bone-forming cells) • Osteoclasts (bone-destroying cells) • Osteogenic cells (stem cells) • Nerve fibers, nutrient blood vessels, and lymphatic vessels enter the bone via nutrient foramina • Secured to underlying bone by Sharpey’s fibers • Endosteum • Delicate membrane on internal surfaces of bone • Also contains osteoblasts and osteoclasts
Endosteum Yellow bone marrow Compact bone Periosteum Perforating (Sharpey’s) fibers Nutrient arteries
Structure of short, irregular and flat bones Spongy bone called diploë in flat bones • Periosteum-covered compact bone on the outside • Endosteum-covers the trabeculae Trabeculae Bone marrow between trabeculae
Location of Hematopoietic Tissue (Red Marrow) • Red marrow cavities of adults • Trabecular cavities of the heads of the femur and humerus • Trabecular cavities of the diploë of flat bones • Red marrow of newborn infants • Medullary cavities and all spaces in spongy bone
Microscopic Anatomy of Bone Osteogenic cell Osteoblast Matrix-synthesizing cell responsible for bone growth Stem cells in periosteum and endosteum that give rise to osteoblasts
Microscopic Anatomy of Bone Osteocyte Osteoclast Mature bone cell that maintains the bone matrix Bone-resorbing cell
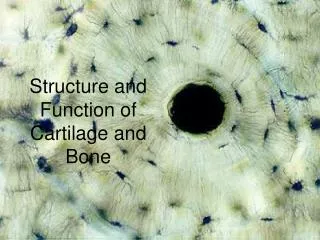
Compact Bone: Haversian system, or osteon—structural unit Artery with capillaries Structures in the central canal Vein Nerve fiber • Central (Haversian) canal • Contains blood vessels and nerves • Lamellae • Weight-bearing • Column-like matrix tubes Lamellae Collagen fibers run in different directions Twisting force
Compact bone Spongy bone Perforating (Volkmann’s) canal: Perpendicular to central canal. Connects blood vessels and nerves of the periosteum with central canal Central (Haversian) canal Osteon Endosteum lining bony canals and covering trabeculae Circumferential lamellae Perforating (Sharpey’s) fibers Periosteal blood vessel Lamellae Periosteum Nerve Vein Lamellae Artery Lacuna (with osteocyte) Central canal Canaliculi Lacunae Osteocyte in a lacuna Interstitial lamellae
Microscopic Anatomy of Bone: Spongy Bone • Trabeculae • Align along lines of stress to resist stress • No osteons • Contain irregularly arranged lamellae, osteocytes, and canaliculi • Capillaries in endosteum supply nutrients
Composition of Bone • Organic • Osteogenic cells, osteoblasts, osteocytes, osteoclasts • Osteoid—organic bone matrix secreted by osteoblasts • Ground substance (proteoglycans, glycoproteins) • Collagen fibers • Provide tensile strength and flexibility • Inorganic • Hydroxyapatites (mineral salts) • 65% of bone by mass • Mainly calcium phosphate crystals • Responsible for hardness and resistance to compression
Bone Development • Osteogenesis (ossification)—bone tissue formation • Stages • Bone formation—begins in the 2nd month of development • Postnatal bone growth—until early adulthood • Bone remodeling and repair—lifelong
Two Types of Ossification • Intramembranous ossification • Membrane bone develops from fibrous membrane • Forms flat bones, e.g. clavicles and cranial bones • Endochondral ossification • Cartilage (endochondral) bone forms by replacing hyaline cartilage • Forms most of the rest of the skeleton
Intramembranous ossification Ossification centers appear in the fibrousconnective tissue membrane. • Selected centrally located mesenchymal cells cluster and differentiate into osteoblasts, forming an ossification center. 1 Collagenfiber Mesenchymalcell Ossificationcenter Osteoid (bone Matrix) Osteoblast 2 Bone matrix (osteoid) is secreted within thefibrous membrane and calcifies.• Osteoblasts begin to secrete osteoid, which is calcified within a few days. • Trapped osteoblasts become osteocytes. Osteoblast Osceocytes Osteoid Newly calcifiedbone matrix
Woven bone and periosteum form. 3 • Osteoid laid down between blood vessels in a random manner. The result is a network of trabeculae called woven bone. • Vascularized mesenchyme condenses and becomes the periosteum. Mesenchyme condensingto form the periosteum Trabeculae ofwoven bone Blood vessel Lamellar bone replaces woven bone, just deep to the periosteum. Red marrow appears. 4 • Trabeculae just deep to the periosteum thicken, and are later replaced with mature lamellar bone, forming compact bone plates. • Spongy bone (diploë), consisting of distinct trabeculae, persists internally and its vascular tissue becomes red marrow. Fibrousperiosteum Osteoblast Plate ofcompact bone 4 Diploë (spongybone) cavitiescontain redmarrow
Endochondral ossification • Uses hyaline cartilage blueprint • Hyaline cartilage breaks down • Before ossification Childhood toadolescence Birth Articularcartilage Secondaryossificationcenter Month 3 Spongybone Week 9 Epiphysealblood vessel Area ofdeterioratingcartilage matrix Epiphysealplatecartilage Hyalinecartilage Spongyboneformation Medullarycavity Bonecollar Bloodvessel ofperiostealbud Primaryossificationcenter 5 1 3 4 2 Cartilage in the center of the diaphysis calcifies and then developscavities. Periosteal bud invades the internal cavities and spongy bonebegins to form. Diaphysis gets longer, medullary cavity forms, ossification continues. 2o ossification center develops. Epiphyses ossify. After, hyalinecartilage is onlyin the epiphysealplates and articularcartilages. Bone collar forms around hyaline cartilagemodel.
Postnatal Bone Growth • How bones widen (appositional growth): • Osteoblasts beneath periosteum secret bone matrix • Osteoclasts on bone surface remove bone • How bones widen • Cartilage divide and hypertrophy and are eventually replaced by bone (see next slide) • Hormonal regulation of bone growth • Growth hormone stimulates epiphyseal plate activity • Thyroid hormone modulates activity of growth hormone • Testosterone and estrogens (at puberty) • Promote adolescent growth spurts • End growth by inducing epiphyseal plate closure
Articular cartilage • GH stimulates the lengthening of bones at the epiphyseal plate. • GH stimulates osteoblast activity & the proliferation of epiphyseal cartilage. • New bone tissue replaces cartilage in this region. • GH stimulates bone thickness by activating osteoblasts under the periosteum. Bone of epiphysis Epiphyseal plate Bone of diaphysis Marrow cavity Cartilage Calcified cartilage Bone
Cartilage Calcified cartilage Bone of epiphysis Resting chondrocytes Bone Chondrocytes undergoing cell division Causes thickening of epiphyseal plate chondrocytes enlarging Epiphyseal plate Calcification of extracellular matrix (chondrocytes die) Dead chondrocytes cleared away by osteoclasts Osteoblasts swarming up from diaphysis and depositing bone over persisting remnants of disintegrating cartilage Diaphysis
Bone remodeling:continuous deposition and resorption of bone • Why? 1. To make bones stronger 2. To maintain Ca 2+ homeostasis • Calcium is necessary for: transmission of nerve impusles, muscle contraction, blood coagulation, secretion by glands, cell division • Primarily controlled by parathyroid hormone (PTH) Blood Ca2+ levels Parathyroid glands release PTH PTH stimulates osteoclasts to degrade bone matrix and release Ca2+ • Blood Ca2+ levels • Calcitonin is secreted by C cells in the thyroid gland to prevent plasma Calcium from being too high
Response to Mechanical Stress • Wolff’s law: A bone grows or remodels in response to forces or demands placed upon it • Observations supporting Wolff’s law: • Handedness (right or left handed) results in bone of one upper limb being thicker and stronger • Curved bones are thickest where they are most likely to buckle • Trabeculae form along lines of stress • Large, bony projections occur where heavy, active muscles attach Load here (body weight) Head of femur Compression here Tension here Point of no stress
Bone fractures may be classified by four “either/or” classifications: • Position of bone ends after fracture: • Nondisplaced—ends retain normal position • Displaced—ends out of normal alignment • Completeness of the break • Complete—broken all the way through • Incomplete—not broken all the way through • Orientation of the break to the long axis of the bone: • Linear—parallel to long axis of the bone • Transverse—perpendicular to long axis of the bone • Whether or not the bone ends penetrate the skin: • Compound (open)—bone ends penetrate the skin • Simple (closed)—bone ends do not penetrate the skin
All fractures can be classified based on these criteria: • Location • External appearance • Nature of the break Some common types of fractures Comminuted: Bone broken into 3 or more pieces. Common in people with brittle bones, such as elderly Compression: Bone is crushed. Common in porous bones (i.e. osteoporotic bone) subjected to fall or other trauma
More types of fractures Depressed: Broken bone is pressed inward. Typical in a skull fracture. Spiral: Ragged break from twisting force on a bone, common in sports injury Greenstick: Bone breaks incompletely, like a broken twig. Only one side of the shaft breaks. Common in kids Epiphyseal: Epiphysis separates from the diaphysis along the epiphyseal plate. Tends to occur where cartilage cells are dying and calcification of the matrix is occurring
Stages in the Healing of a Bone Fracture Internalcallus(fibroustissue andcartilage) Externalcallus Hematoma Newbloodvessels Spongybonetrabecula 1 A hematoma forms. Fibrocartilaginouscallus forms. 2 Bonycallus ofspongybone Healedfracture 4 Bone remodeling occurs. 3 Bony callus forms.
Homeostatic Imbalances • Osteomalacia and rickets • Calcium salts not deposited • Rickets (childhood disease) causes bowed legs and other bone deformities • Cause: vitamin D deficiency or insufficient dietary calcium • Paget’s disease • Excessive and haphazard bone formation and breakdown, usually in spine, pelvis, femur, or skull • Pagetic bone has very high ratio of spongy to compact bone and reduced mineralization • Unknown cause (possibly viral) • Treatment includes calcitonin and biphosphonates
Osteoporosis • Loss of bone mass—bone resorption outpaces deposit • Spongy bone of spine and neck of femur become most susceptible to fracture • Risk factors: Lack of estrogen, calcium or vitamin D; petite body form; immobility; low levels of TSH; diabetes mellitus Treatment and prevention: • Calcium, vitamin D, and fluoride supplements • Weight-bearing exercise throughout life • Hormone (estrogen) replacement therapy slows bone loss • Some drugs (Fosamax, SERMs, statins) increase bone mineral density
Developmental Aspects of Bones • Embryonic skeleton ossifies predictably so fetal age easily determined from X rays or sonograms • At birth, most long bones are well ossified (except epiphyses) • Nearly all bones completely ossified by age 25 • Bone mass decreases with age beginning in 4th decade • Rate of loss determined by genetics and environmental factors • In old age, bone resorption predominates