Download
1 / 38
380 likes | 620 Views
PHARMAC, Pharmaceutical Schedule and Subsidy for Medicines and Special Foods. Zaheer-Ud-Din Babar, PhD Senior Lecturer in Pharmacy Practice School of Pharmacy, FMHS, University of Auckland z.babar@auckland.ac.nz. Objectives. To understand pharmaceutical reimbursement in New Zealand

E N D
PHARMAC, Pharmaceutical Schedule and Subsidy for Medicines and Special Foods Zaheer-Ud-Din Babar, PhD Senior Lecturer in Pharmacy Practice School of Pharmacy, FMHS, University of Auckland z.babar@auckland.ac.nz
Objectives • To understand pharmaceutical reimbursement in New Zealand • To understand why medicines are listed on the Pharmaceutical Schedule • To understand the role of PHARMAC, the use of Special authority and Consideration of Schedule H.
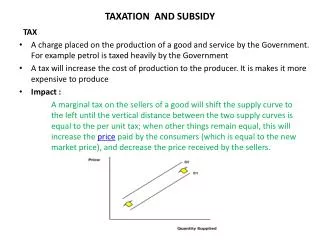
Medicines Costs • Pharmaceutical costs are a major driver of health care expenditure. • During recent years drug expenditure has risen faster than other healthcare costs in many countries. REASONS • New high-priced drugs • Emerging resistant microbes • Increase in life expectancy • Increased more demand for speciality treatment/products by patients Source: Garc´ıa-Alonso MDC, Mari˜noso BG. The strategic interaction between firms and formulary committees: Effects on the prices of new drugs. Journal of Health Economics 27 (2008) 377–404
Why to learn reimbursement and pricing of pharmaceuticals? Image Credit: Medicines New Zealand , 2007 Unlimited needs-Resources are limited Governments have to find ways to rationalise the use of medicines. Low availability and high prices could be the major barriers towards Access to Medicines
How to improve access and affordability? • Regulate Markets (Control Prices) • Due to the distortion in the market forces, most governments seem to think that regulation of the pharmaceutical market is necessary in order to secure appropriate quality, safety and efficacy of medicines. • Compulsory Health Insurance/Subsidy by the government • Governments would also like to ensure that the population have access to important medicines ( independent of patients/consumers ability to pay) • Reimbursement for Medicines • Agencies have been set up to decide which drugs are value for money (= Pharmacoeconomics) • The National Institute for Clinical Excellence (NICE) in the UK • Pharmaceutical Management Agency of New Zealand (Pharmac) • Pharmaceutical Benefits Advisory in Australia • Commission of Transparency in France.
Expenditures on Pharmaceuticals as % of total Expenditures on Health Source: OECD Health Data 2008 – Version June 2008http://www.oecd.org/dataoecd/46/36/38979632.xls.
Per capita spending on medicines in Australia, New Zealand, Canada and the United States • Source: Calculations based on data from OECD Health Data 2008. Figures are expressed in Australian dollars using the general purchasing power parity indices to convert currencies. • * New Zealand data for public spending on prescription drugs from PHARMAC, Annual Review 2006, www.pharmac.govt.nz/suppliers/reports/AnnualReview.
Impact of PHARMAC on drug expenditure Source: PHARMAC
New Zealand Pharmaceutical Market Publicly-funded hospital pharmaceuticals Publicly-funded community pharmaceuticals Privately-funded pharmaceuticals (Source: Pharmac 2009)
PHARMAC • Established in 1993, the Pharmaceutical Management Agency of New Zealand (PHARMAC) works within a fixed budget for public spending on medicines in New Zealand. • Fixed budget means that PHARMAC has to prioritise spending ( trade-off between different treatment options) • PHARMAC uses this budget, along with a variety of supplier contracts, to act as a national purchaser of medicines. • Manage pharmaceutical budget on behalf of DHBs Source: Morgan & Boothe (2009) Prescription drug coverage in Australia and New Zealand: a view from afar- Australian Prescriber http://www.australianprescriber.com/magazine/33/1/2/4
PHARMAC • Once a drug is approved for sale in New Zealand, drug companies can apply to PHARMAC for it to be government funded. • PHARMAC’s key roles are to decide whether a medicine will be subsidised, the price the government is prepared to pay, and the conditions of access. • Negotiate prices with pharmaceutical manufacturers • Single purchaser of pharmaceuticals (PHARMAC) • Monopoly purchasing = low prices! • Subsidisation of new drugs is tightly controlled • Pharmac uses rebates on list prices, tendering of off-patent drugs, bundle agreements (where PHARMAC may list expensive new drugs in return for the manufacturer discounting the price of other products it supplies) • Pharmac also uses access restrictions (special authorities) and reference pricing to contain expenditures Source: Morgan & Boothe (2009) Prescription drug coverage in Australia and New Zealand: a view from afar- Australian Prescriber http://www.australianprescriber.com/magazine/33/1/2/4
How PHARMAC works? • In community settings, only drugs on the pharmaceutical schedule receive government subsidy. • For the drugs which are not subsidised, New Zealanders have to pay out of pocket. • Patients generally make a co-payment for each medicine listed in the schedule that they get dispensed. • The consumers may need to pay an additional fee if the subsidy level PHARMAC has set is less than the price charged by the pharmaceutical company. Cumming J, Mays N, DaubéJ. How New Zealand has contained expenditure on drugs. BMJ 2010; 340:c2441 doi: 10.1136/bmj.c2441 http://www.bmj.com/content/340/7758/Analysis.full.pdf
How PHARMAC works? • PHARMAC uses a well documented process to determine which drugs are added to the pharmaceutical schedule • When a company applies to PHARMAC for government funding for a new drug it submits information on the costs and benefits. • This information is assessed by PHARMAC’s Pharmacology and Therapeutics Advisory Committee (PTAC), which advises whether the medicine should be subsidised or not (However, PHARMAC is not bound to accept PTAC’s recommendations). Cumming J, Mays N, DaubéJ. How New Zealand has contained expenditure on drugs. BMJ 2010; 340:c2441 doi: 10.1136/bmj.c2441 http://www.bmj.com/content/340/7758/Analysis.full.pdf
Pharmacology and Therapeutics Advisory Committee (PTAC) • PTAC is an expert medical committee which provides independent advice to PHARMAC on health needs and the clinical benefits of particular pharmaceuticals for use in the community and/or in DHB Hospitals. • PTAC helps decide which community pharmaceuticals are to be subsidised from public monies by making recommendations to PHARMAC. • PHARMAC may obtain clinical advice from PTAC in relation to national purchasing strategies for Hospital Pharmaceuticals. • PTAC has number of subcommittees • There may be additional specialist hospital representatives on PTAC subcommittees • One of the subcommittee is the Special Foods Subcommittee Source: Pharmaceutical Schedule, January 2011, Volume 18 Number 0 http://www.pharmac.govt.nz/2011/01/01/Schedule.pdf
PHARMAC’s criteria for deciding funding for a particular medicines • Health needs of the population • Specific health needs of Maori and Pacific peoples • Availability of existing medicines, treatment devices, and related products • Clinical benefits and risks • Cost effectiveness of meeting health needs by funding the drug rather than using other publicly funded health and disability support services • Budgetary impact of any changes to the pharmaceutical schedule • Direct cost to health service users • Government’s priorities for health funding • Such other criteria as PHARMAC thinks fit (after appropriate consultation) Source: PHARMAC. Operating policies and procedures of the pharmaceutical management agency (“PHARMAC”). 2006. http://www.pharmac.govt.nz/2005/12/22/231205.pdf
Pharmac has following functions under Section 103 of the Crown Entities Act • To maintain and manage a pharmaceutical schedule including determining eligibility and criteria for the provision of subsidies. • To manage exceptional circumstances scheme ( to provide for subsidies for the supply of pharmaceuticals not on the pharmaceutical schedule) • To promote the responsible use of pharmaceuticals; • To manage the purchasing of any or all pharmaceuticals, whether used either in a hospital or outside it, on behalf of DHBs). • In exceptional circumstances providing for subsidies for the supply of pharmaceuticals not listed on the Pharmaceutical Schedule. Source: Pharmaceutical Schedule, January 2011, Volume 18 Number 0 http://www.pharmac.govt.nz/2011/01/01/Schedule.pdf
PHARMAC manages the National Pharmaceutical Schedule Community Pharmaceuticals • The Schedule lists medicines available in the community and subsidised by the Government with funding from the Pharmaceutical Budget • In the community approximately 1848 Pharmaceuticals are subsidised by the Government. • Community pharmaceuticals are listed as Sections A to G of the Pharmaceutical Schedule Hospital Pharmaceuticals • The schedule also lists medicines which are purchased by DHBs for use in their hospitals. • This also includes those hospital medicines for which national prices have been negotiated by PHARMAC. • Section H is allocated for Hospital Pharmaceuticals Source: Pharmaceutical Schedule, January 2011, Volume 18 Number 0 http://www.pharmac.govt.nz/2011/01/01/Schedule.pdf
Section H of Pharmaceutical Schedule • Section H of the Pharmaceutical Schedule includes Pharmaceuticals that can be purchased at a national price by DHBs for use in their hospitals. DHBs can also negotiate pricing with suppliers. • These are referred to as National Contract Pharmaceuticals. • Section H also identifies new pharmaceuticals used in hospitals, which have been assessed by PHARMAC ( the results of this analysis is being available to DHB Hospitals via PHARMAC’s website). • Section H of the Pharmaceutical Schedule also list medicines which DHBs can fund from their own budgets for use in the community: • These medicines do not need a specific Hospital Exceptional Circumstances approval. • These medicines are not are not subsidised from the Pharmaceutical Budget as Community Pharmaceuticals. • Source: Pharmaceutical Schedule, January 2011, Volume 18 Number 0 http://www.pharmac.govt.nz/2011/01/01/Schedule.pdf
Section H of Pharmaceutical Schedule Section H lists Pharmaceuticals that DHBs fund from their own budgets. The Hospital Pharmaceuticals are grouped into the following Parts in Section H: • Part I lists the rules in relation to Hospital Pharmaceuticals. • Part II lists Hospital Pharmaceuticals for which national contracts exist (National Contract Pharmaceuticals). • These are listed alphabetically by generic chemical entity name and line item, the relevant Price negotiated by PHARMAC and, if applicable, an indication of whether it has Hospital Supply Status (HSS) and any associated Discretionary Variance (DV) Pharmaceuticals and DV Limit. Source: Pharmaceutical Schedule, January 2011, Volume 18 Number 0 http://www.pharmac.govt.nz/2011/01/01/Schedule.pdf
Section H: Hospital Pharmaceuticals • Part III lists Assessed Pharmaceuticals, which have been or are being assessed by PHARMAC. (However, DHB Hospitals are not obliged to implement those recommendations. • Part IV lists Discretionary Community Supply Pharmaceuticals, which are not Community Pharmaceuticals, but which a DHB Hospital can, in its discretion, fund for use in the community from its own budget. • The index located at the back of the Section H supplement can be used to find page numbers for generic chemical entities, or product brand names, for Hospital Pharmaceuticals. Source: Pharmaceutical Schedule, January 2011, Volume 18 Number 0 http://www.pharmac.govt.nz/2011/01/01/Schedule.pdf
How to access data from schedule? • PHARMAC has set up an interactive Schedule on the internet http://www.pharmac.govt.nz. • It can be used to calculate the cost of a prescribed Community Pharmaceutical. The site takes into account the following: • The quantity of Community Pharmaceutical prescribed • The patient’s age • Whether the patient has a community services card, high use health card or prescription subsidy card, the fee for pharmacy services and prescription charges. • Other information on PHARMAC website includes: • Copies of the Annual Review • Annual Report and Annual Plan • Pharmaceutical Schedule, Pharmaceutical Schedule Updates, National Hospital Pharmaceutical Strategy, other publications and recent press releases. Source: Section H for Hospital Pharmaceuticals Nov 2010. http://www.pharmac.govt.nz/2010/10/28/SectionH.pdf
Special Authority • Special Authority is an application process in which a prescriber requests government subsidy on a Community Pharmaceutical for a particular person. • The particular person must be eligible according to the access criteria. • Applications must be submitted to the Ministry of Health by the prescriber for the request to be processed. Source: Pharmaceutical Schedule, January 2011, Volume 18 Number 0 http://www.pharmac.govt.nz/2011/01/01/Schedule.pdf
Special Authority Applications • Once approved, the prescriber will be provided a Special Authority number which must appear on the prescription. • Specialists who make an application must communicate the valid authority number to the prescriber who will be writing the prescriptions. • The authority number can provide access to subsidy, increased subsidy, or waive certain restrictions otherwise present on the Community Pharmaceutical. • Some approvals are dependent on the availability of funding from the Pharmaceutical Budget. Source: Pharmaceutical Schedule, January 2011, Volume 18 Number 0 http://www.pharmac.govt.nz/2011/01/01/Schedule.pdf
How special foods are funded? • Pharmacology and Therapeutics Advisory Committee (PTAC) • Special Foods Subcommittee • Often the decisions are made by using reference pricing • PHARMAC gets the following information from the PTAC subcommittee: • What is current practice? • What is the clinical trial evidence for the new product and how does it compare with other available products? • How much additional benefit does the new product provide? ( Acknowledgement: PHARMAC, 2011)
What is reference pricing? • In reference pricing, medicines/products are classified into clusters based on similar therapeutic effects. • The payer sets a reference price (RP) for each cluster based on a relatively low priced product - for example, the minimum or median price -- in the cluster. Source:Danzon PM, Ketcham JD. Reference Pricing of Pharmaceuticals for Medicare: Evidence from Germany, the Netherlands and New Zealand. NBER Working Paper No. 10007 September 2003 JEL No. I11, I18, L11, L51 http://www.econ.canterbury.ac.nz/personal_pages/john_fountain/econ337/reading/danzonrefpricing.pdf
Reference pricing in New Zealand Woodfield A, Fountain J, Borren P, Money and Medicines. An Economic Analysis of Reference Pricing and Related Public-sector Cost-containment Systems for Pharmaceuticals with Special Reference to New Zealand, Merck Sharp & Dome, New Zealand, 1997. Morton FS. The strategic response by pharmaceutical firms to Medicaid most-favoured-customer rules. Rand Journal of Economics 1997;28(2):269–90.
Example of reference pricing- Elecare • Elemental formula is used for the dietary management of children with severe cow’s milk allergy and multiple food protein intolerance. • The funding of Elecare has been considered by the Special Foods Subcommittee of PTAC. • The Special Foods Subcommittee recommended that Elecare be listed in the Pharmaceutical Schedule if cost neutral compared to currently listed elemental formula products. Proposal relating to the funding of various Special Foods 30th July 2010 http://www.pharmac.govt.nz/2010/07/30/2010-07-30%20Consultation%20on%20various%20Special%20Food%20funding%20proposals.pdf
When to apply reference pricing? • In addition the Subcommittee considered that Elecare has the same or similar clinical effect to Neocate and Neocate Advance and that these products should be included in the same reference price group. • The Subcommittee considered that as these products had a similar clinical effect and that reference pricing was appropriate. (If two products have the same clinical effect then Pharmac would maintain that only the cheapest should be funded)
Appendix 1 ( Special Foods, Vitamins, Minerals, Oral electrolyte replacement products )
Special Food Details on Schedule • From page 176 of the Pharmaceutical Schedule, January 2011 (224 pages, 1270 KB) • SA0585 – Adult Products High Calorie: Two Cal HN • SA0702 – Adult Products Standard 1.0 kcal/ml : Ensure Plus, Fibresource, Fortisip, Isosource, Jevity, Nutrison, Osmolite, Resource Plus • SA0702 Adult Products Standard 1.5 kcal/ml [ Isosoucre 1.5, Ensure Plus RTH, Nutrison Energy Multifibre] • SA0581 – Carbohydrate and Fat: Duocal Super Soluble Powder • SA0912 – Carbohydrate: Moducal, Morrex Maltodextrin, Polycal, Polycose • SA0588 – Respiratory Products- CORD Products: Pulmocare • SA0594 – Diabetic Products: Diasip, Diason, Glucerna, Glucerna RTH, Resource Diabetic, Resource Diabetic RTH • Source: Pharmaceutical Schedule, January 2011, Volume 18 Number 0http://www.pharmac.govt.nz/2011/01/01/Schedule.pdf
Special Food Details on Schedule • SA0615 – Fat Modified Products: Monogen • SA0899 – Fat: Calogen, Liquigen, MCT oil (Nutricia) • SA0595 – Food Thickeners: Karicare Food Thickener, Resource Thicken Up • SA0732 – Foods used for Homocystinuria or maple syrup urine disease: Maxamaid MSUD, Maxamum MSUD, MSUD Aid, XMET Maxamum • SA0733 – Foods used for PKU: Aminogran Food Supplement, Aminogran Mineral Mix, Analog LCP, Aproten, Loprofin, Loprofin Mix, Maxamaid XP, Maxamum XP, Minaphlex, Phlexy 10 • SA0722 – Gluten Free Foods: Gluten Free Bread Mix 100% Bakels, Healtheries Wheat and Gluten Free Baking, Horleys Bread Mix, Horleys Flour, NZB • Source: Pharmaceutical Schedule, January 2011, Volume 18 Number 0http://www.pharmac.govt.nz/2011/01/01/Schedule.pdf
Special Food Details on Schedule • SA0589 – High Protein Products: Fortimel • SA0603 – Infant Formulae – For Gastrointestinal And Other Malabsorptive Problems: Elecare, Neocate, Pepti Junior, Vivonex Pediatric • SA0604 – Infant Formulae – For Milk Intolerance: Delact, S26 Soy, Karicare Goats Milk Infant Formula • SA0602 – Infant Formulae – For Premature Infants: S26LBW, Similac Special Care • SA0601 – Infant Formulae – For Williams Syndrome: Locasol • SA0757 – Infant Formulae – Lactose Intolerance and Cows’ Milk Protein Intolerance: Karicare All Ages • SA0962 – Metabolic Mineral Mixture • SA0583 – Oral Supplements: Ensure, Sustagen Hospital Formula Source: Pharmaceutical Schedule, January 2011, Volume 18 Number 0http://www.pharmac.govt.nz/2011/01/01/Schedule.pdf
Special Food Details on Schedule • SA0607 – Paediatric Product For Children Awaiting Liver Transplant: Generaid Plus • SA0606 – Paediatric Product For Children With Chronic Renal Failure: Kindergen • SA0896 – Paediatric Products: Nutrini, Pediasure (1 page, 3 KB) • SA0586 – Products for Undialysed End Stage Renal Failure: Suplena • SA0582 – Protein: Protifar 90, Promod, Resource Beneprotein • SA0587 – Renal Products: Nepro, NovaSource Renal, Nutrison Concentrated RTH, Renilon 7.5 • SA0592 – Specialised And Elemental Products: Alitraq, Elemental 028 Extra, Peptisorb RTH, Vital HN, Vivonex TEN Source: Pharmaceutical Schedule, January 2011, Volume 18 Number 0 http://www.pharmac.govt.nz/2011/01/01/Schedule.pdf
Vitamin Products • Vitamin A with Vitamin D and C ( solution 1000 u with Vitamin D 400 u and ascorbic acid 300 mg per 10 drops) • Pyridoxine hydrochloride (Tab 25 mg or Tab 50 mg) • Thiamine hydrochloride ( Tab 50 mg) • Vitamin B Complex (Tab strong BPC) • Ascorbic acid (Tab 100 mg) • Alpha tocopheryl acetate (water solubilised solution 156 iu/ml) • Multivitamins (tab or powder or oral liquid) • Vitamins (fat soluble vitamins A,D, E, K)
Mineral Products • Calcium carbonate (tab 1.25 g ( 500 mg elemental) or tab 1.5 g (600 mg elemental) or tab 1.75 g ( 1 g elemental) • Sodium fluoride (Tab 1.1 mg (0.5 mg elemental) • Ferrous fumarate (Tab 200 mg ( 65 mg elemental) • Ferrous fumarate with folic Acid (Tab 310 mg ( 100 mg elemental) with Folic acid 350 ug • Ferrous sulphate ( tab long acting 325 mg (105 mg elemental) • Ferrous sulphate with folic acid (tab long acting 325 mg (105 mg elemental with folic acid 350 ug
Oral electrolyte replacement products • Compound electrolytes ( powder for solution for oral use 5 g) • Dextrose with electrolytes ( solution with electrolytes) • Potassium bicarbonate ( Tab eff 315 mg with sodium acid phosphate 1.937 g and sodium bicarbonate 350 mg) • Potassium Chloride ( Tab eff 584 mg (14 m eq) with chloride 385 mg (8 m eq) or tab long acting 600 mg
Acknowledgement • I would like to thank PHARMAC for giving comments on earlier drafts of this presentation.