Download
1 / 38
380 likes | 390 Views
INFLAMMATON OF THE LIVER. Hepatitis A-B Viruses part І. Dr. Osama AL Jiffri. HEPATITIS A VIRUS. HEPATITIS VIRUS. Hepatitis A-B-D-C-F-E Hepatitis A and E Viruses do not persist in the liver There is no evidence of progression to chronic liver damage

E N D
Hepatitis A-B Virusespart І Dr. Osama AL Jiffri
HEPATITIS VIRUS • Hepatitis A-B-D-C-F-E • Hepatitis A and E Viruses do not persist in the liver • There is no evidence of progression to chronic liver damage • Hepatitis B, D, C, may be associated with persistent infection and progression to chronic liver disease
Hepatitis A Virus: Structure and Classification • Picornavirus • genus : Hepatovirus • Member of the Enterovidae • Offcially referred to as enterovirus 72 • The virions have cubic symmetry and are 27nm • Naked icosahedral capsid • SS RNA (7400 nucleotides) • Single serotype worldwide • Humans only reservoir
HEPATITIS A VIRUS TRANSMISSION Fecal-oral transmission Mode: • Close personal contact(e.g., household contact, sex contact, child day-care centers) • Contaminated food, water(e.g., infected food handlers, contaminated raw oysters)
Hepatitis A: Pathogenesis • Incubation 4 weeks (range 2-6 weeks) • Particularly in young children • Replicates in hepatocytes (little damage to cells) released via bile to intestines 7-10 days prior to clinical symptoms
Hepatitis A: Clinical Features-1 • An acute illness with: • Clinical illness usually starts with a few days of malaise, loss of appetite, fatigue, abdominal pain, nausea, vomiting) • jaundice or elevated serum aminotransferase (AST, ALT) levels, dark urine, light stool • Adults usually more symptomatic • Patients are infective while they are shedding the virus in the stool- usually before the onset of symptoms • Complete recovery 99% (rarely can be fulminant)
EVENTS IN HEPATITIS A VIRUS INFECTION Clinical illness Infection ALT IgM IgG Viremia Response HAV in stool 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Week
Hepatitis A Diagnosis • Detection of anti HAV IgM antibody by an ELISA or Radioimmunoassay test • Liver enzyme test
PREVENTING HEPATITIS A • Hygiene (e.g., hand washing) • Sanitation (e.g., clean water sources) • Immune globulin (pre- and post-exposure) (older passive vaccination) • Hepatitis A vaccine (pre-exposure)
Hepatitis A Treatment • Supportive- no specific role of antiviral therapy • Lifelong immunity likely after infection or vaccination
HEPATITISA VACCINES 1st dose at time 0 2nd dose 6-12 months afterwards
Hepatitis A Vaccine • Vaccine is recommended for the following persons 2 years of age and older: • Travelers to areas with increased rates of hepatitis A - Persons with chronic liver disease • Children living in areas with increased rates of hepatitis A
Hep A : Passive Immunization • Hepatitis A immune globulin can be given up to 2 weeks after an exposure • Immunity temporary (4-5 months) • Also given in travelers leaving for endemic area on short notice (ie not enough time for the vaccine to be effective)
HBV: Structure • Family : Hepadnaviridae (Hepatitis DNA viruses) • complete virion • 42nm enveloped virus and double-shelled Dane particle • (consist only of excess surface antigen) • Hepatitis B core antigen (HBcAg) • Hepatitis B e antigen (HBeAg) • Genome consists Circular double stranded DNA • Length of 3200 nucleotides • Virus stable and resist environmental factors
HBV: Epidemiology • Worldwide Distribution • Acute and Chronic infections 1. Center for Disease Control CDC and HI Vand Hepatitis.com, 2002
Geographic Distribution of Chronic HBV Infection HBsAg Prevalence ³8% - High 2-7% - Intermediate <2% - Low
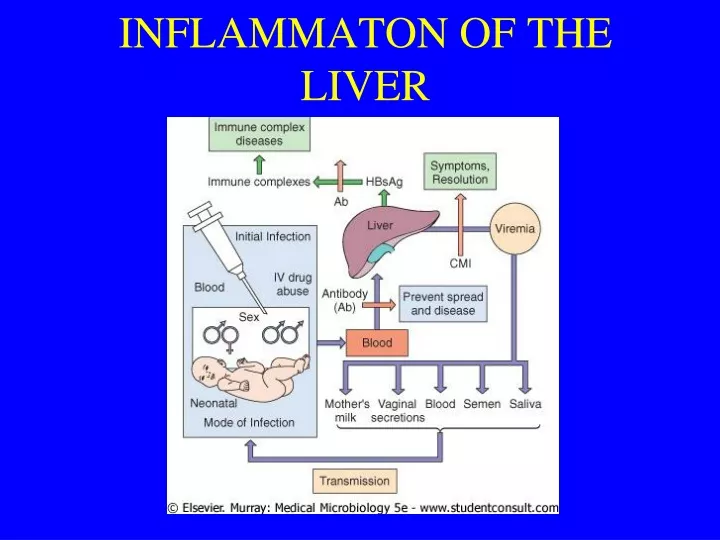
Hepatitis B Virus in Various Body Fluids Low High Moderate blood semen urine serum vaginal fluid feces wound exudates saliva sweat tears breast milk
Risk Factors for Acute Hepatitis B Heterosexual* (41%) Injecting Drug Use (15%) Homosexual Activity (9%) Household Contact (2%) Health Care Employment (1%) Unknown (31%) Other (1%)
HBV Pathogenesis • Virus enters hepatocytes via blood • Immune response (cytotoxic T cell) responsible for clinical syndrome • 5 % of adults become chronic carriers (HBsAg> 6 months) • Higher rate of hepatocellular carcinoma in chronic carriers, • Hepatitis B surface antibody likely confers lifelong immunity • Hepatitis B e Ag indicates high transmissibility • Hepatitis B e Ab indicates low transmissibility
Hepatitis B - Clinical Features • Incubation period: Average 60-90 days • Clinical illness (jaundice): less common in • young children • Acute case-fatality rate: 0.5%-1% • Chronic infection: <5 yrs, 30%-90%³5 yrs, 2%-10% • ( More likely in asymptomatic infections) • 15 to 25% of chronically infected patients will die from chronic liver disease
Possible Outcomes of HBV Infection Acute hepatitis B infection 95% of infant-acquired infections 3-5% of adult-acquiredinfections Chronic HBV infection Chronic hepatitis 12-25% in 5 years Cirrhosis 20-23% in 5 years 6-15% in 5 years Hepatocellularcarcinoma Liver failure Death Death
Acute Hepatitis B Virus Infection with Recovery Typical Serologic Course Symptoms anti-HBe HBeAg Total anti-HBc Titer anti-HBs IgM anti-HBc HBsAg 0 4 8 12 16 24 28 32 52 100 20 36 Weeks after Exposure
Progression to Chronic Hepatitis B Virus Infection Typical Serologic Course Acute (6 months) Chronic (Years) HBeAg anti-HBe HBsAg Total anti-HBc Titer IgM anti-HBc Years 0 4 8 16 20 24 28 36 12 32 52 Weeks after Exposure
Current Treatment Options for HBV • Interferon alfa (Intron A) • Lamivudine (Epivir HBV) • Adefovir dipivoxil (Hepsera)
Control of Hepatitis B • Prevent perinatal HBV transmission • (HBs Ag screening of pregnant women) • Routine vaccination of all infants • Vaccination of children, adolescents, and adults in high-risk groups
Hepatitis B Vaccine • Infants: several options that depend on status of the mother • If mother HBsAg negative: birth, 1-2m,6-18m • If mother HBsAg positive: vaccine and Hep B immune globulin within 12 hours of birth, 1-2m, <6m • Adults • 0,1, 6 months • Vaccine recommended in • All those aged 0-18 • Those at high risk
Hepatitis B High Risk Groups • Persons with multiple sex partners or diagnosis of a sexually transmitted disease • Men who have sex with men • Sex contacts of infected persons • Injection drug users • Household contacts of chronically infected persons • Infants born to infected mothers • Infants/children of immigrants from areas with high rates of HBV infection • Health care and public safety workers • Hemodialysis patients
Hepatitis B: Passive Immunization • Infants of surface antigen positive mothers • Exposures to infected blood or infected body fluids in individuals who are unvaccinated, unknown vaccination, or known non-responders. • Ideally within 24 hours • Probably not effective >7days post exposure
www.kau.edu.sa/ojiffri الملفات