Download
1 / 41
480 likes | 1.02k Views
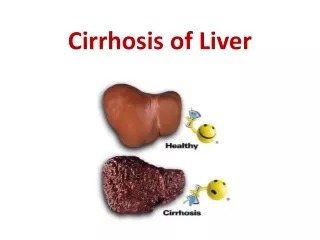
Cirrhosis of the Liver. Hepatic Cirrhosis. It is a chronic progressive disease characterized by: - replacement of normal liver tissue with diffuse fibrosis that disrupts the structure and function of the liver. Extensive parenchymal cell degeneration Destruction of parenchymal cells.

E N D
Hepatic Cirrhosis • It is a chronic progressive disease characterized by: - replacement of normal liver tissue with diffuse fibrosis that disrupts the structure and function of the liver • Extensive parenchymal cell degeneration • Destruction of parenchymal cells
Etiology and Pathophysiology • Four types of cirrhosis: • Alcoholic (Laennec’s) cirrhosis • Postnecrotic cirrhosis • Biliary cirrhosis • Cardiac cirrhosis
Etiology and Pathophysiology A. Alcoholic or Laennec’s Cirrhosis • In which the scar tissue characteristically surrounds the portal areas • This is the most frequently caused by chronic alcoholism, common type of cirrhosis • Preceded by a theoretically reversible fatty infiltration of the liver cells
B. Post necrotic cirrhosis • Complication of toxic or viral hepatitis • Accounts for 20% of the cases of cirrhosis • Broad bands of scar tissue form within the liver • Etiology and Pathophysiology
C. Biliary Cirrhosis • In which scarring occurs in the liver around the bile ducts. • This type of cirrhosis usually results from chronic biliary obstruction and infection (cholangitis) • Accounts for 15% of all cases of cirrhosis • Etiology and Pathophysiology
Etiology and Pathophysiology D. Cardiac Cirrhosis • Results from longstanding severe right-sided heart failure
Diagnostic Finding 1. serum albumin • Decrease in level 2. liver enzymes • SGPT(ALT),SGOT(AST) increases 3.Serum bilirubin • Increases 4. Prothrombin time • prolong
5. Ultrasound scanning • Used to measure the difference in density of parenchymal cells and scar tissue. 6. CT-scan, MRI • It gives information about liver size, hepatic blood flow and obstruction 7. Liver biopsy 8.ABG • May reveal a ventilation-perfusion imbalance and hypoxia
Clinical ManifestationsEarly Manifestations • Onset usually insidious • GI disturbances: • Anorexia • Dyspepsia • Flatulence • N-V, change in bowel habits
Clinical ManifestationsEarly Manifestations • Abdominal pain • Fever • Lassitude • Weight loss • Enlarged liver or spleen
Clinical ManifestationsLate Manifestations • Two causative mechanisms • Hepatocellular failure • Portal hypertension
Clinical ManifestationsJaundice • Occurs because of insufficient conjugation of bilirubin by the liver cells, and local obstruction of biliary ducts by scarring and regenerating tissue
Clinical ManifestationsJaundice • Intermittent jaundice is characteristic of biliary cirrhosis • Late stages of cirrhosis the patient will usually be jaundiced
Clinical ManifestationsSkin • Spider angiomas (telangiectasia, spider nevi) • Palmar erythema
Clinical ManifestationsEndocrine Disturbances • Steroid hormonesof the adrenal cortex (aldosterone), testes, and ovaries are metabolized and inactivated by the normal liver
Clinical ManifestationsEndocrine Disturbances • Alteration in hair distribution • Decreased amount of pubic hair • Axillary and pectoral alopecia
Clinical ManifestationsHematologic Disorders • Bleeding tendencies as a result of decreased production of hepatic clotting factors (II, VII, IX, and X)
Clinical ManifestationsHematologic Disorders • Anemia, leukopenia, and thrombocytopenia are believed to be result of hypersplenism
Clinical ManifestationsPeripheral Neuropathy • Dietary deficiencies of thiamine, folic acid, and vitamin B12
Steatorrhea • Fatty stool • The passage of abnormally increase amounts of fats in the feces (more than 5g/day) due to reduced absorption of fat by intestine • The feces are pale, smell offensive, look greasy
Pruritus • Due to biliary obstruction leading to retention of bile salts. • Patients may develop vascular spider angiomas on the skin usually above the waistline • These are numerous small vessels resembling a spider’s leg
Complications • Portal hypertension and esophageal varices • Peripheral edema and ascites • Hepatic encephalopathy • Hepato-renal Syndrome
ComplicationsPortal Hypertension • Characterized by: • Increased venous pressure in portal circulation • Splenomegaly • Esophageal varices • Systemic hypertension
ComplicationsPortal Hypertension • Primary mechanism is the increased resistance to blood flow through the liver
ComplicationsPortal HypertensionSplenomegaly • Back pressure caused by portal hypertension chronic passive congestion as a result of increased pressure in the splenic vein
ComplicationsPortal HypertensionEsophageal Varices • Increased blood flow through the portal system results in dilation and enlargement of the plexus veins of the esophagus and produces varices
ComplicationsPortal HypertensionEsophageal Varices • Varices have fragile vessel walls which bleed easily
ComplicationsPortal HypertensionInternal Hemorrhoids • Occurs because of the dilation of the mesenteric veins and rectal veins
ComplicationsPortal HypertensionCaput Medusae • Collateral circulation involves the superficial veins of the abdominal wall leading to the development of dilated veins around the umbilicus
ComplicationsPeripheral Edema and Ascites • Ascites: - Intraperitoneal accumulation of watery fluid containing small amounts of protein
ComplicationsPeripheral Edema and Ascites • Factors involved in the pathogenesis of ascites: • Hypoalbuminemia • Levels of aldosterone • Portal hypertension
ComplicationsHepatic Encephalopathy • Liver damage causes blood to enter systemic circulation without liver detoxification
ComplicationsHepatic Encephalopathy • Main pathogenic toxin is NH3 although other etiological factors have been identified • Frequently a terminal complication
ComplicationsFetor Hepaticus • Musty, sweetish odor detected on the patient’s breath • From accumulation of digested by-products
Hepatorenal syndrome • acute renal failure coupled with advanced hepatic disease (due to cirrhosis or less often metastatic tumor or severe alcoholic hepatitis) • characterized by: • Oliguria • benign urine sediment • very low rate of sodium excretion • progressive rise in the plasma creatinine concentration
Hepatorenal Syndrome • Reduction in GFR often clinically masked • Prognosis is poor unless hepatic function improves • Nephrotoxic agents and overdiuresis can precipitate HRS
Diagnostic Studies • Liver function tests • Liver biopsy • Liver scan • Liver ultrasound
Diagnostic Studies • Esophagogastroduodenoscopy • Prothrombin time • Testing of stool for occult blood