Download
1 / 1
10 likes | 129 Views
Smoking Cessation in DOTS Clinics in Rio de Janeiro Enhancing tuberculosis treatment through smoking cessation

E N D
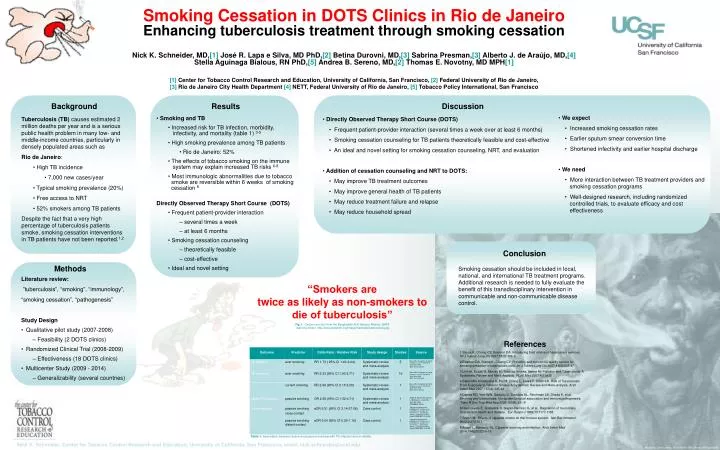
Smoking Cessation in DOTS Clinics in Rio de Janeiro Enhancing tuberculosis treatment through smoking cessation Nick K. Schneider, MD,[1] José R. Lapa e Silva, MD PhD,[2] Betina Durovni, MD,[3] Sabrina Presman,[3] Alberto J. de Araújo, MD,[4] Stella Aguinaga Bialous, RN PhD,[5] Andrea B. Sereno, MD,[2] Thomas E. Novotny, MD MPH[1] [1]Center for Tobacco Control Research and Education, University of California, San Francisco, [2] Federal University of Rio de Janeiro, [3] Rio de Janeiro City Health Department [4] NETT, Federal University of Rio de Janeiro, [5] Tobacco Policy International, San Francisco Conclusion Smoking cessation should be included in local, national, and international TB treatment programs. Additional research is needed to fully evaluate the benefit of this transdisciplinary intervention in communicable and non-communicable disease control. Background Results Discussion • We expect • Increased smoking cessation rates • Earlier sputum smear conversion time • Shortened infectivity and earlier hospital discharge • We need • More interaction between TB treatment providers and smoking cessation programs • Well-designed research, including randomized controlled trials, to evaluate efficacy and cost effectiveness • Tuberculosis (TB) causesestimated 2 million deaths per year and is a serious public health problem in many low- and middle-income countries, particularly in densely populated areas such as • Rio de Janeiro: • High TB incidence • 7,000 new cases/year • Typical smoking prevalence (20%) • Free access to NRT • 52% smokers among TB patients • Despite the fact that a very high percentage of tuberculosis patients smoke, smoking cessation interventions in TB patients have not been reported.1,2 • Smoking and TB • Increased risk for TB infection, morbidity, infectivity, and mortality (table 1) 3-5 • High smoking prevalence among TB patients • Rio de Janeiro: 52% • The effects of tobacco smoking on the immune system may explain increased TB risks 6-8 • Most immunologic abnormalities due to tobacco smoke are reversible within 6 weeks of smoking cessation 8 • Directly Observed Therapy Short Course (DOTS) • Frequent patient-provider interaction • several times a week • at least 6 months • Smoking cessation counseling • theoretically feasible • cost-effective • Ideal and novel setting • Directly Observed Therapy Short Course (DOTS) • Frequent patient-provider interaction (several times a week over at least 6 months) • Smoking cessation counseling for TB patients theoretically feasible and cost-effective • An ideal and novel setting for smoking cessation counseling, NRT, and evaluation • Addition of cessation counseling and NRT to DOTS: • May improve TB treatment outcomes • May improve general health of TB patients • May reduce treatment failure and relapse • May reduce household spread Methods • Literature review: • ”tuberculosis”, “smoking”, “immunology”, • “smoking cessation”, “pathogenesis” • Study Design • Qualitative pilot study (2007-2008) • Feasibility (2 DOTS clinics) • Randomized Clinical Trial (2008-2009) • Effectiveness (18 DOTS clinics) • Multicenter Study (2009 - 2014) • Generalizability (several countries) “Smokers are twice as likely as non-smokers to die of tuberculosis” Fig.1: Cartoon and text from the Bangladesh Anti-Tobacco Alliance, BATA (warning sticker, http://bata.globalink.org/image/materials/tuberculosis.jpg) References 1 Slama K, Chiang CY, Enarson DA. Introducing brief advice in tuberculosis services. Int J Tuberc Lung Dis 2007;11(5):496-9 2 Enarson DA, Slama K, Chiang CY. Providing and monitoring quality service for smoking cessation in tuberculosis care. Int J Tuberc Lung Dis 2007;11(8):838-47. 3Lin HH, Ezzati M, Murray M. Tobacco Smoke, Indoor Air Pollution and Tuberculosis: A Systematic Review and Meta-Analysis. PLoS Med 2007;4(1):e20 4 Bates MN, Khalakdina A, Pai M, Chang L, Lessa F, Smith KR. Risk of Tuberculosis From Exposure to Tobacco Smoke: A Systematic Review and Meta-analysis. Arch Intern Med 2007;167(4):335-42 5 Davies PD, Yew WW, Ganguly D, Davidow AL, Reichman LB, Dheda K, et al. Smoking and tuberculosis: the epidemiological association and immunopathogenesis. Trans R Soc Trop Med Hyg 2006;100(4):291-8 6 Houtmeyers E, Gosselink R, Gayan-Ramirez G, et al. Regulation of mucociliary clearance in health and disease. Eur Respir J 1999;13:1177-1188 7 Sopori M. Effects of cigarette smoke on the immune system. Nat Rev Immunol 2002;2:372-377 8 Arcavi L, Benowitz NL. Cigarette smoking and infection. Arch Intern Med 2004;164(20):2206-16 Table 1: Association between active and passive smoking with TB infection and morbidity Nick K. Schneider,Center for Tobacco Control Research and Education, University of California, San Francisco, email: nick.schneider@ucsf.edu Mural by John Lewis, 1810 North 16th Street, Philadelphia






















