Download
1 / 39
560 likes | 1.36k Views
Paget Disease. Stephanie Kimbrel Diane Morris Heather Sloan. Sir James Paget. Paget Disease. Osteitis Deformans Second most common bone disease after osteoporosis . Bones Most Commonly Involved . Pelvis Femur Tibia Spine Skull. Epidemiology. Viral: Measles

E N D
Paget Disease Stephanie Kimbrel Diane Morris Heather Sloan
Paget Disease Osteitis Deformans Second most common bone disease after osteoporosis
Bones Most Commonly Involved Pelvis Femur Tibia Spine Skull
Epidemiology • Viral: Measles Respiratory Syncytial Virus (RSV) Slow Virus (paramyxoviruses): present for years before symptoms appear
Epidemiology • Genetic 15% to 40% of persons with the disease have a first-degree relative with the disease, numerous studies also show other relatives with the disease • Sequestrosomel 1(one) gene on chromosome 5
Demographics/Cultural Considerations First appeared in Western Europe populations with the earliest documented cases dating back to the Roman and Anglo-Saxon periods in England Closely parallels patterns of migration from Western Europe
Demographics/Cultural Considerations Patients with a family history are more likely to have parents born in Europe than those with sporadic disease New England has the highest number of patients with the disease
Demographics/Cultural Considerations Disease is uncommon before the age of 40 By the age of 80, 1 out of 10 persons is affected 18% to 25% of the US population have one family member with Paget Disease
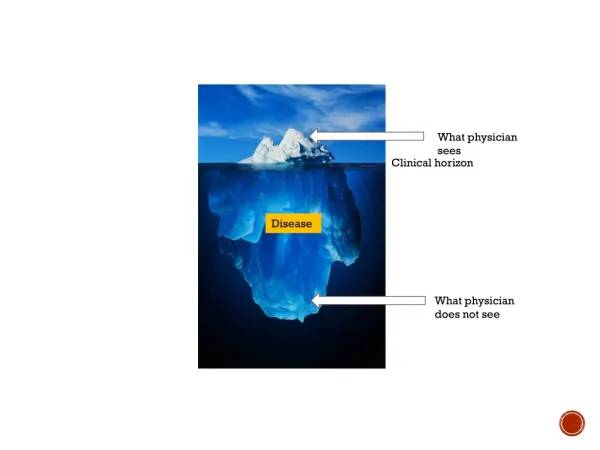
Paget Disease: Definition Paget’s disease of the bone is a focal disorder of chaotic bone remodeling with increased osteoblastic and osteoclastic activity that results in disorganized woven and lamellar bone in one or more skeletal sites. End result is bone of poor quality that is enlarged, hypervascular, and susceptible to deformation and fracture
Anatomy and Physiology OSTEOBLASTS OSTEOCLASTS *Functions in building *Functions in the the osseous matrix of breakdown of the bone the bone matrix
Pathophysiology • Increased osteoclastic numbers • Osteoclastic are abnormal in size and activity with excessive nuclei. • Leads to voids and cavities in the bone • Followed by chaotic bone formation by osteoblasts. • New bone is woven vs. lamellar • “Collage of mosaic matrix” • Hypervascularity
Pathophysiology • Mineralization rates are normal • Bone remodeling normally: 10-15% of bone surfaces • May increase five to ten fold. • Cortex= increases its porosity and blurs the distinction between cortical and cancellous bone • Newly formed bone is not organized and irregular • Bone enlargement • Deformity
Three Phases: Phase One Initial short lived burst of multinucleate osteoclastic activity causing bone resoprtion During this phase there is a marked elevation of serum alkaline phosphate (SAP)
Phase Two A mixed phase of both osteoclastic and osteoblastic activity with increased levels of bone turnover leading to deposition of structurally abnormal bone Excessive activity=deformities
Phase Three Final chronic sclerotic phase during which the bone formation outweighs bone resportion Combined with old age leads to arthritis Can lead to chronic non-specific inflammation and occasional narrowing of the foramens
Differential Diagnosis Osteoarthritis Gout Pseudogout Osteomalacia
Osteoarthritis • Prevalence increases with age • Involves the entire joint • Most commonly affected joints are the hands, knee, hip, hands, and lumbar & cervical spine • Presents with joint pain and stiffness: worse with activity • A degenerative joint disorder • Result of mechanical and biologic events that destabilize the normal process of degradation and synthesis of articular cartilage chondrocytes, extracellular matrix, and subchondral bone
Key diagnostic criteria X-ray’s reveal new bone formation, joint space narrowing, and subchondral sclerosis and cysts Pain associated with activities, weight-bearing joints being associated with weight-bearing activities Pain at rest or at night is unusual (except with advanced OA) Functional difficulties Commonly involved joint HANDS, knee, hip, and lumbar & cervical spine Bouchard nodes (PIP) and Heberden nodes (DIP) Limited ROM, both limited and active Bony malalignment
Gout • A syndrome characterized by: • Hyperuricemia • Deposition of urate crystals causing attacks of acute inflammatory arthritis • Tophi around the joints • And possible joint destruction
Key diagnostic criteria Arthrocentesis with synovial fluid analysis Uric acid level: men >7mg/dL, women >6mg/dL X-ray reveals periarticular erosions (overhanging edge or punched-out appearance Men aged 40-60 years Use of gout-inducing medication Consumption of meat, seafood, or alcohol Rapid-onset of severe pain Joint stiffness Few affected joints Swelling and joint effusion Tenderness Tophi Foot joint distribution Erythema and warmth Family hx
Pseudogout CLINICAL PRESENTATION • Acute Attack: • Monoarticular attacks: knee • Joint inflammation, pain, heat, redness of the swelling, and chills • Proximal muscle pain Acute synovitis caused by calcium pyrophosphate dihydrate crystals.
Key diagnostic criteria Arthrocentesis with presence of weakly positive birefringent rhomboid shaped crystals. ( yellow perpendicular and blue parallel to polarizer axis) Synovial fluid should be analyzed. Plain radiographs often reveal chondrocalcinosis located parallel to subchondral bone: knee menisci, wrist triangular fibrocartilage and symphisis pubis Generally affects older people and both men and women equally
Osteomalacia A metabolic bone disease characterized by incomplete mineralization of the underlying mature organic bone matrix following growth plate closure in adults. Rickets is a different manifestation of the same underlying pathologic process. (Buttaro, T.M., Trybulski, J., Bailey, P.P., Sandberg-Cook, J. , 2008; Holick, M.F. , 2007)
Key diagnostic criteria • Primarily vitamin D deficiency. • No differentiating s/s yet osteomalacia is more likely to present with s/s of bony tenderness and pain. Diagnostics - Elevated serum 25 hydroxyvitamin D levels (normal in Paget disease) • Elevated total serum alkaline phosphatase level (normally markedly elevated in Paget disease) • Normal serum calcium in Paget disease • X-ray shows gross deformities of bone such as enlargement of the skull in Paget disease (Holick, M.F. , 2007; Van Staa, T.P., Selby, P., Leufkens, H.G., et al. , 2002; Whitehouse, R.W. ,2002)
When to treat? Extensive or symptomatic disease; neurological complications; serum alkaline phosphatase level 3-4 times normal; weight bearing bones, skull, or vertebrae involvement. Goal is to prevent progression by suppressing osteoclastic activity which allows the osteoblasts to catch up and lay normal bone (Buttaro, T.M., Trybulski, J., Bailey, P.P., Sandberg-Cook, J., 2008; Ferri, F., 2012)
Treatment options 1.) Calcium and vitamin D 2.) Oral Bisphosphonates (alendronate [Fosamax], risedronate [Actonel]) 3.) IV Bisphosphonates ( pamidronate [Aredia], zoledronic acid [Zometa]) 4.) Calcitonin 5.) Pain management- Acetaminophen, ASA, NSAIDS (Buttaro, T.M., Trybulski, J., Bailey, P.P., Sandberg-Cook, J., 2008; Ferri, F., 2012)
Follow up Disease activity is monitored by biochemical markers (SAP or NTx) measured q 3-6 months in active disease or yearly in inactive disease Assess pain, joint symptoms, neurologic function, and medication side effects every visit. Refer to orthopedics/neurosurgery when an arthropathy or spinal stenosis causes unremitting pain or function loss. (Buttaro, T.M., Trybulski, J., Bailey, P.P., Sandberg-Cook, J., 2008; Ferri, F., 2012)
Paget’s Disease at a Glance Paget's disease is a chronic bone disorder. Paget's disease frequently causes no symptoms. Paget's disease can cause pain in the bones or joints, headaches and hearing loss, pressure on nerves, increased head size, bowing of limb, or curvature of spine. Tests used to diagnose Paget's disease include X-rays, blood tests, and bone scanning. Paget's disease can lead to other medical conditions. Medical treatment options include aspirin, other anti-inflammatory medications, pain medications, and medications that slow the rate of bone turnover, decreasing the activity of Paget's disease. Surgical operations may necessary for damaged joints, fractures, severely deformed bones, or when nerves are being pinched by enlarged bone.
Question Which bones are most commonly involved in Paget’s Disease? a) Skull b) Spine c) Tibia d) Femur e) Pelvis f) All of the above
Question What does the word osteoblasts mean? a) Functions in the building of the osseous matrix of the bone b) Functions in the breaking down of the bone c) Neither
Question What lab is elevated when trying to rule out a diagnosis for Paget’s Disease? a) Uric Acid b) Serum Alkaline Phosphate (SAP) c) Hydroxyvitamin D level
References • Ansiello & Goldman (2004). Cicil Textbook of Medicine (22nd ed.). Philidelphia, PA: Saunders • Buttaro, T.M., Trybulski, J., Bailey, P.P., Sandberg-Cook, J. (2008). Primary Care: A Collaborative Practive (3rd ed.). St. Louis, MO: Mosby • Ferri, F. (2012). Ferri’s Clinical Advisor. Providence, Rhode Island: Mosby. • Holick, M.F. (2007). Vitamin D Deficiency. New England Journal of Medicine, 357, 266-281 • Matfin, G., Mattson Porth, C., (2009). Pathophysiology-Concepts of Altered Health States (8th ed.). Philadelphia, PA: Wolters Kluwer & Lippincott Williams & Wilkins. • Thompson, J.C. (2010). Netter’s Concise Orthopaedic Anatomy (2nd ed.). Philidelphia, PA: Saunders • Van Staa, T.P., Selby, P., Leuflkens, H.G., et al. (2002). Incidence and Natural History of Paget’s Disease of Bone in England and Wales. Bone Miner, 17, 465-471. • Whitehouse, R.W. (2002). Paget’s Disease of Bone. Semin Musculoskeletal Radiol, 6, 313-322
Photography References http://emedicine.medscape.com/article/394165-overview#a01 http://www.google.com/search?q=pictures+of+osteoclast&hl=en&qscrl=1&nord=1&rlz=1T4ADRA_enUS432US433&prmd=imvns&tbm=isch&tbo=u&source=univ&sa=X&ei=4y1YT5ynHs3DsQLL48WvDQ&ved=0CCIQsAQ&biw=1366&bih=627 http://www.google.com/search?q=pictures+of+osteoblasts&hl=en&qscrl=1&nord=1&rlz=1T4ADRA_enUS432US433&prmd=imvns&tbm=isch&tbo=u&source=univ&sa=X&ei=5kVYT529AuOssQKU_endDQ&ved=0CC8QsAQ&biw=1366&bih=627 http://www.mayoclinic.com/health/pagets-disease-of-bone/DS00485 http://en.wikipedia.org/wiki/Paget's_disease_of_bone http://osteoarthritis.about.com/od/osteoarthritis101/ss/explained_8.htm http://www.gout-aware.com/gout-and-pseudogout.html